In a scathing opinion, California’s First District Court of Appeals found that the California Department of Corrections and Rehabilitation has showed “deliberate indifference” to the health of people imprisoned at San Quentin State Prison outside San Francisco. A three-judge panel found that the department violated the Eighth Amendment’s prohibition on cruel and unusual punishment when it failed to immediately follow public health experts’ recommendation to halve the prison’s population. The court ordered CDCR officials to reduce the prison’s population to 1,775 people in order to allow for more social distancing inside its grounds. The corrections department could downsize the prison by releasing prisoners or transferring them to other state prisons.
Twenty-eight prisoners died and about three-quarters of the people incarcerated in San Quentin became infected with the coronavirus this summer after untested prisoners from a Southern California prison struggling with its own outbreak were brought in. In early June, after the first handful of prisoners there tested positive, public health experts toured the prison and issued an urgent memo calling for its population to be reduced by half as soon as possible.
“By all accounts, the COVID-19 outbreak at San Quentin has been the worst epidemiological disaster in California correctional history. And there is no assurance San Quentin will not experience a second or even third spike,” Presiding Justice J. Anthony Kline wrote in the opinion. “Failure to immediately adopt and implement measures designed to eliminate double celling, dormitory style housing and other measures to permit physical distancing between inmates is morally indefensible and constitutionally untenable.”
As I reported this summer, San Quentin was particularly vulnerable to an outbreak due to its age, design, and crowding:
In the North and West cell blocks, which hold about 1,600 people—including 300 with four or more COVID-19 risk factors, according to the public health experts—windows are welded shut. Air is recirculated among five tiers of two-person cells, passing freely through grates or bars that open onto narrow walkways. James King, an activist with the Ella Baker Center who was released from San Quentin in December, describes the North and West cell blocks as “concrete boxes” where illness routinely spread in waves. “We used to joke and call it that we were living in a petri dish,” King says.
The lower-security dormitories at San Quentin are also packed, as is a gymnasium filled with rows of bunks that the public health experts said was at a high risk for a “catastrophic super spreader event.” Prisoners in the dorms share toilets, sinks, showers, and phones. (CDCR says that access to phone calls, and showers is staggered to allow for disinfecting between each use.) “I got one person who lives about eight inches away from my face,” says Kerry Rudd, who lives in a San Quentin dorm of about 100 people. “And of course the person on the bunk below me, he lives about four feet from me.”
As of October 14, CDCR had reduced the number of people incarcerated in San Quentin’s to 2,898, in part through a series of release programs announced by Gov. Gavin Newsom in July. In his order, Kline recommended the state further expand its release programs to include prisoners serving time for “a violent crime as defined by law.” That could potentially include some of the roughly 30 percent of San Quentin prisoners serving life sentences.
“Given the length of their minimum sentences, lifers are much older than non-violent offenders at the time they become eligible for parole and receive a release date,” Kline wrote in his order. “Most have by then ‘aged out’ of criminal behavior and present less of a threat to public safety.”
In a statement to Politico, a representative for the state corrections department said it “respectfully disagree[s] with the court’s determination, as CDCR has taken extensive actions to respond to the COVID-19 pandemic” and added that the state currently has its lowest prison population in “decades.” The court’s order takes effect on November 4.
As colder weather sets in, experts are warning that the next coronavirus surge has arrived. On Friday, the United States recorded 69,000 new infections—the highest daily total since July 30. This latest peak is concentrated in rural communities in the upper Midwest and follows a spring surge in the Northeast and a summer surge in the South. Experts are now worried about a rising number of cases coinciding with flu season as families gather indoors during the holiday season and winter months.
“There’s a growing sense of coronavirus fatigue out there,” Dr. William Schaffner, an epidemiologist at Vanderbilt University, told CNBC. “People really want to get back to the old normal.” But ignoring public health guidelines could have dire consequences; some states are already feeling the impacts of the latest surge in cases.
In Wisconsin, Democratic Gov. Tony Evers opened up a field hospital for coronavirus patients with more moderate symptoms to ease the crowding in intensive care units in the state’s hospitals. North Dakota’s case load has reached record highs and state officials are beginning to worry about hospital capacity. In Minnesota, where 18 cases were associated with a Donald Trump campaign event, coronavirus infections have also reached new highs.
The latest surge comes just weeks before the election. The Trump administration remains wholly uncommitted to responding to the coronavirus, even as the president’s poll numbers sink, in part, due to his handling of the pandemic. Even as deaths top 217,000 and the third wave threatens to be worse than the first two, Trump continues to downplay the severity of the virus. “The light at the end of the tunnel is near,” he told a crowd of supporters in Florida on Friday. “We are rounding the turn.”
Allison Mulattieri as Told To Will PeischelOctober 13, 2020
Mother Jones Illustration
We asked people who have quit since January 2020 how and why they did it. You can read more about the project, and the initial nine stories, here. Got your own quitting tale? Send us an email.
Allison Mulattieri, 38
Position: Cashier, TJX Marshalls Retail Started: December 2004 Quit: July 2020 Salary: $12.00 per hour, approximately $20,000 per year (started at $8.50 per hour)
As told to Will Peischel
I worked at Marshalls in Boston, where I live, as a cashier for about 15 years.
In the middle of March everything really started closing down. We had a couple of months of paid furlough. We were all at home. The store was entirely closed. Then, around May they started getting ready to reopen.
Things were still pretty crazy in terms of the pandemic. As soon as the city allowed people to go back though, Marshalls then set a hard date for the reopening. I believe it was June 11. After 30 days without taking shifts, I’d be considered a non-return, and automatically punted.
I wanted to extend my leave a little more, so I wouldn’t have to come back immediately. I wanted to wait until the beginning of the fall. I was allowed, by store benefit, up to 60 days of announced leave. According to benefits, I had it.
I spoke to a manager. They said, “You have to file through the online portal that you’ve been checking in with us this whole time.” So, I filed through that. Two weeks later, when I spoke to a separate manager, they said that this wasn’t even the right way to go about it. I had to talk to the company HR directly.
They were putting me through this rigmarole to see if I was willing to come back—because if I wasn’t they’d find somebody else. I felt like they had boxed me into that decision. Basically, I was given a fake task to keep me satisfied—or give me the illusion of doing something—until it became a make or break situation where I had to say, “I’m coming back now,” or “I’m quitting.” It was like they only told me then, after the furlough, I got the answer: “We won’t certify this leave.”
I finally got fed up and said, “I’m not coming back.”
After I gave my resignation, I was penduluming between relief but also a kind of guilt. On the one hand, I was relieved that I was able to make this choice and ensure my own safety. But at the same time, I felt this terrible guilt. You’re doing this after 15 years, you’re giving up this job you were doing. You have other coworkers in that job coming back. What makes you better than them?
I saw one of my coworkers on the train as I was going somewhere. I don’t know if she didn’t recognize me or didn’t want to talk to me. I wonder if they feel like I’ve abandoned them. I’d worked there for 15 years, and I’d kind of gotten used to it as much as you can. It did feel a lot like Stockholm syndrome. Am I going into a situation full of even more unknowns than the one I’m leaving?
Right now, I’m trying to figure out what I’m going to do. On the good days when I’m able to calm down the guilt and anxiety, I feel like this is kind of liberating because I’ve been doing some things I’ve always wanted to do. I’ve been trying to learn Japanese through Duolingo and those online learning programs, and now I have a chance to really focus on it even more because my mental load isn’t as taxed.
And, there’s more time to work on my art. I’ve been a fan of Japanese animation since high school. About the time that I started my job of 15 years, I was also taken as a volunteer for Boston’s anime convention, Anime Boston. I liked to illustrate and draw comics in my free time, and I showed them some examples of my work. They asked me to start drawing designs for them. Could you draw pictures of our convection mascots? Could you provide designs for merchandise we have for the convention?We have branded tumblers, keychains, patches, and pins. They really like the look that I did for patches and pins, and I’ve been doing a patch and collectible pin design for them every single year. That’s been my main legacy from working for them.
I was thinking, if there was a way I could turn this art I do for free into something more self-supporting, could I become a freelance artist because I have the time to support myself? As per my anxiety and my guilty personality, I never really felt I was good enough to make a job out of the art I’d do online or for this convention. If the convention has had me for 15 years, maybe what I produce as an artist is good enough to start charging?
I really have to keep telling myself things aren’t over just yet. Maybe it’s time to look at something more—what I want—than what I just need to get by.
President Trump made his first in-person appearance at a hastily organized White House event on Saturday, less than two weeks after he tested positive for the coronavirus. His doctors have been cagey about the seriousness of his illness and refuse to answer questions about when the president last tested negative for the virus. Despite being hospitalized for three days—with several of his top advisers also infected including Stephen Miller and campaign manager Bill Stepien—Trump hopped back on the denial train. His first stop? Pandering to Black people.
It’s not uncommon for candidates to make last-minute pleas to voters who may be undecided. But what made Trump’s late-in-the-game pitch so damning is that the effects of his administration’s bungling pandemic response and relentless efforts to downplay the severity of the virus have fallen disproportionately on the very people he’s now reaching out to. Trump, who has refused to publicly recognize or mourn the victims, has also never acknowledged the role that race plays in the inequality of the disease. Not even when his top Black surrogate died of it in July.
Herman Cain, whose 2012 presidential run was a precursor to Trump’s first campaign, was perhaps Trump’s most well-known Black supporter. The former pizza mogul became chair of the Black Voices for Trump coalition, a group that seeks to promote Trump’s policies to Black voters. Ever loyal, Cain blogged and tweeted in support of Trump during the pandemic and denied science right alongside him. In June, less than two weeks after he was photographed without a mask at a rally in Tulsa, Oklahoma, Cain fell ill and was hospitalized. Meanwhile, throughout his hospital stay, his public relations team kept tweeting how the 74-year-old cancer survivor was improving and the virus was not a big deal. (Sound familiar?) They praised a professional baseball team for not panicking about an outbreak “like the media wanted.”
Less than a month after he announced he’d been infected, Herman Cain died from the coronavirus. Because the campaign does not engage in contact tracing, the public will never know if Cain contracted the virus from attending the rally, but the timing and the optics left little doubt.
Even the death from COVID of a high-profile Black Trump supporter did not spur a Republican reckoning. Aside from calling Cain a “great friend” on the day of his death, I can’t recall the president or any high-ranking staffer either paying their respects or mentioning what killed him. At the first presidential debate last month, the president even insisted that holding rallies were safe. When the moderator, Fox News‘ Chris Wallace, asked him if he was worried about the virus spreading at his campaign events, Trump responded, “Well, so far we have had no problem whatsoever.” (Herman Cain, who?) Last week, Minnesota officials announced that nine coronavirus cases can be linked to a Trump rally last month. Two of the sick have been hospitalized.
Meanwhile, Cain’s PR team has kept his Twitter account alive. They’re still tweeting in support of Trump’s COVID response.
It’s no surprise that Trump’s rally for voters of color was completely divorced from reality. The event, which was billed as a “peaceful protest for law enforcement,” was organized by Candace Owens, a popular conservative pundit who heads Blexit, an organization that focuses on convincing Black people to leave the Democratic Party and join the Republican cause. That effort, already a near-impossibility, became downright delusional when Trump used his first public appearance to pander to Black and Brown voters without even mentioning the disproportionate toll the coronavirus has taken on our communities.
“I recently announced my plan to deliver more opportunity, security, fairness, and prosperity to the Black community, to the Hispanic community,” Trump said from the White House balcony in front of a small crowd. But the coronavirus has stripped away anything resembling security, fairness, or prosperity in communities of color.
He praised law enforcement, touted an economic recovery that is simply not happening, and continued to lie about the virus saying it would disappear, as he has insisted since the spring. Too bad it didn’t disappear before 215,000 people, including Cain, died from it.
According to the American Public Media Research Lab, nearly one in 1,000 Black Americans have died from COVID. Latinx and Indigenous communities have also suffered disproportionately and are more likely to die from the virus than their white counterparts. And though it’s generally thought that young children are largely unaffected, 75 percent of the children who have died from the coronavirus have been children of color.
The current state of affairs is bleak for Americans of all races, as tens of thousands of people test positive every day and Trump continues to downplay the public health crisis and play politics with our lives—and his. According to a report from Axios, the president would like to be out on the road every single day until the election, despite the risks to himself, everyone close to him, and those who attend his rallies. As one aide told Axios, “He’s going to kill himself.” Trump is scheduled to appear in Florida on Monday night.
It might be too much to ask a racist president to care about an outsize Black death toll. But it’s tragic that a top Black surrogate like Cain remains so easily erased from Trump’s fantastical narrative. It’s the perfect metaphor for the pandemic response overall. Ignore Cain’s death and pretend the Trump administration’s coronavirus strategy is a success. Ignore the disproportionate toll the virus has taken on the Black community and pretend your presidency is Black America’s second coming. “I’ve done more for the Black community than any president since Abraham Lincoln,” Trump said (not for the first time) at Saturday’s White House event. “Nobody can dispute it.”
Nine cases of coronavirus have been linked with a rally held by President Donald Trump on September 18 in Bemidji, Minnesota. Health officials told Minnesota Public Radio that two of the nine people have been hospitalized, with one requiring intensive care.
Trump’s campaign attempted to downplay any connection to the cases. “Tying these cases to an outdoor event that occurred three weeks ago, where hand sanitizer and face masks were supplied, is a stretch,” campaign spokesperson Tim Murtaugh told The Hill. “We wish them all speedy recoveries.”
While Joe Biden has suspended large campaign rallies in line with Centers for Disease Control recommendations, Trump has eschewed the warnings of his own administration’s scientists, continuing to hold events indoors and outdoors with hundreds of people. On most occasions, he has refused to wear a mask himself, and has mocked Biden for doing so and otherwise following experts’ recommendations. Last week, the president announced that he had contracted COVID-19, but the White House has declined to provide details on the timing or outcome of his test results. The president continued attending events with supporters after he was exposed and potentially was contagious, including another Minnesota rally on September 30.
The Bemidji event was not the first and will not be the last Trump rally to be linked to the spread of COVID. Former GOP presidential primary candidate Herman Cain, a prominent Trump supporter, died of COVID in July, weeks after attending a rally in Tulsa, Oklahoma, which the city’s top health official said was likely associated with a local spike in diagnoses. The Federal Emergency Management Agency has documented that the recent White House event formally announcing his nomination of Amy Cohen Barrett to the Supreme Court, where hundreds of Republican leaders socialized and sat closely outdoors mostly without masks, has already been been linked to 34 cases.
Minnesota’s cases have steadily climbed since September, in concert with the nation’s general failure to keep the disease in check. The United States is now reporting its highest number of daily COVID-19 infections since mid-August, with 57,420 new positives Friday—the third consecutive day of more than 50,000 reported cases—according to Johns Hopkins University. More than two dozen states are now reporting steadily increasing cases.
Some health officials are particularly worried Florida will soon reemerge as a hot spot. “What they’ve done is opened up everything as if nothing had ever happened there and you and I could be talking probably in eight to 10 weeks, and I will likely bet that Florida will be a house on fire,” Mike Osterholm, director of the Center for Infectious Disease Research and Policy at the University of Minnesota told CNN on Friday.
Despite his illness and continued speculation he could still be contagious, the superspreader-in-chief plans to hold his next swing-state rally on Monday, just a week after he was hospitalized. The location? Sanford, Florida.
In an interview with CBS News, Dr. Anthony Fauci stated plainly what many people had suspected: The largely mask-free gathering at the White House to celebrate Amy Coney Barrett’s nomination to the Supreme Court was a “superspreader event.”
After Fauci explained to CBS’s Steven Portnoy the importance of wearing masks given that asymptomatic people can spread the virus, Portnoy pointed that the White House’s prevention strategy relied on routine testing rather than mask usage. “What did we learn about the efficacy of that strategy in terms of preventing the spread of coronavirus?” he asked.
“Well, I think the data speak for themselves,” Fauci replied. “We had a superspreader event in the White House, and it was in a situation where people were crowded together and were not wearing masks.”
In the interview, Fauci also said that Trump’s repeated use of the word “cure” to refer to the therapeutic treatments he’d received could lead to “confusion.” “I think you really have to depend on what you mean by a ‘cure,'” he said. “We have good treatments for people with advanced disease who are in the hospital.”
When the markets rebounded, so did the most fortunate.Getty
When America started going into pandemic lockdown back in March, the situation was scary and uncertain for rich and poor alike. The wealthy feared that their industries, investment portfolios, and personal fortunes would be greatly diminished. Low- and middle-income people feared that their jobs and pantries would dry up, that they would be evicted and foreclosed upon. With prospects now fading for a pre-election stimulus bill and the Trump administration’s promise of a V-shaped recovery yet to materialize, America’s most vulnerable remain fearful. But our richest citizens are enjoying a strong comeback.
Earlier this week, Wealth-X, an analytics firm that crunches data on the world’s most fortunate people, released its World Ultra Wealth Report 2020. The report covers 2019 mainly, but it includes a section on how ultra-high net worth individuals—those with net assets of $30 million or more—have fared during the pandemic.
Very well, thanks. Economically, things were looking pretty fabulous for this elite group before COVID came calling. As of 2019, the United States, with about 4 percent of the planet’s population, boasted more than 32 percent of the world’s ultrawealthy individuals. From 2016 to 2019, America’s ultrawealthy set grew by 28 percent, to 93,790 people, while their combined assets grew to more than $11 trillion—an even bigger increase.
Then came coronavirus. From the end of 2019 through the end of March 2020, Wealth-X reports, the combined ultrawealthy populations of the US and Canada plummeted by 23 percent. Almost 24,000 folks dropped out of that elite category. But the performance of the equities markets do not reflect the lived reality of most people, and those in the highest tiers tend to obtain most of their income from investments. When the markets rebounded, so did the most fortunate. By the end of August 2020, America’s ultra-high-net-worth population was back to where it was on January 1, and their overall wealth was down less than 1 percent for 2020—not bad, considering the year before had been an unusually profitable one for this particular demographic.
At first, the pandemic threw quite a twist into the book I’ve been working on these past two years. Titled Jackpot, it digs into the experiences of America’s wealthiest citizens in an age of near-Dickensian economic inequality, and how our relentless urge to accumulate affects our society. Having done most of my reporting pre-COVID, I had to reconnect with all my wealthy sources to see how the crisis was affecting them. Some were understandably fearful for both their fellow citizens and personal fortunes, but it soon became clear that most would do just fine—if not exceedingly well, as so many of America’s billionaires have.
One source, the founder of a successful technology company that went public and was later acquired for more than $1 billion in current dollars, had just closed a fresh funding round on one of two startups he’d seeded. The other startup, a point-of-care diagnostics company, quickly pivoted to COVID testing. “We got lucky,” he said, and more personally, “as it turns out, I had a lot of cash.” So his financial advisors were helping him find promising moneymaking opportunities in the down market.
Another ultrawealthy source, whose industry faced an “existential” crisis, he told me, soon realized that the situation could prove very profitable for his private equity portfolio (so long as his industry recovered within a few years). A third, who also had lots of cash on hand when the markets tanked in the spring, used the opportunity to invest in companies that stood to profit from the pandemic, and short-sold the broader market as a hedge, a play that may yet pay off.
According to Wealth-X, nearly 38 percent of the wealth held by the planet’s richest people is in liquid form: cash, income, and dividends. This liquidity, and ready access to capital, are among the perks of the well-heeled. They enable a person to pounce on juicy business opportunities even as the underlying economy is screwing the pooch.
The government has taken care of the wealthy, too. Lobbyists slipped provisions into the CARES Act that amount to a tax break of more than $160 billion that will largely benefit the kinds of folks I’ve been interviewing. “Nice provisions,” one responded when I described the new tax breaks; “What the fuck?” replied another. I called up Steven Rosenthal, a tax attorney and senior fellow at the Urban-Brookings Tax Policy Center. Rosenthal, who used to work for Congress’ Joint Committee on Taxation, was vehemently opposed to this bailout for the ultrawealthy. “The owner society is really doing quite well through the government’s help,” he told me. “The way I look at it is you’ve got capitalism for gains and socialism for losses.”
The privileged few who can afford to hire lobbyists were “genuinely scared about losing businesses and wiping out a good chunk of their fortune. I understand that,” Rosenthal added. “But their fright is not the same kind of fright as people who are going to be thrown out on the street.”
President Trump’s first on-air interview since testing positive for the coronavirus will include a televised “medical evaluation” performed by a Fox News contributor who has repeatedly spread misinformation about COVID-19. The stunt, which will be aired on “Tucker Carlson Tonight” Friday, follows Trump’s insistence that he’s safe to resume public events despite having been admitted to Walter Reed Medical Center, where he received a serious treatment for the coronavirus, one a week ago.
But as experts warn that it’s nearly impossible to know if Trump is still contagious with the deadly disease so soon after contracting it, the president is now apparently relying on Dr. Marc Siegel, the author of the forthcoming COVID: the Politics of Fear and the Power of Science, to impart a false show of medical professionalism in order to back his demands to get back on the campaign trail. As I wrote in March, Siegel was one of three supposed experts that appeared alongside the president for a misinformation-filled Fox News town hall on the coronavirus. (Talk show doctor Mehmet Oz and Dr. Nicole Saphier, also frequent guests on the network, were included.) Since the start of the pandemic, all three have pushed medical advice contradicting public health officials and the Centers for Disease Control and Prevention.
“They are a bunch of alarmists, they are saber rattlers,” Siegel had said during a Fox News appearance on March 6. “There’s no reason to believe it’s actually more problematic or deadly than influenza.” In between promoting hydroxychloroquine, praising the president’s abysmal response to the virus, and downplaying Trump’s diagnosis, Siegel also interviewed Trump in July when the president bragged about performing well on his cognitive assessment. “You go, ‘person, woman, man, camera, TV,'” Trump told Siegel in a moment that was widely ridiculed. “They say, ‘That’s amazing. How did you do that?'”
The on-air evaluation on Friday will come amid overwhelming skepticism over Trump’s condition, after his doctor, Dr. Sean Conley, admitted to lying about the president’s condition in order to publicly reflect an upbeat attitude. Conley on Thursday declared Trump safe to return to public engagements starting Saturday, the same day Trump wants to hold a rally in Florida.
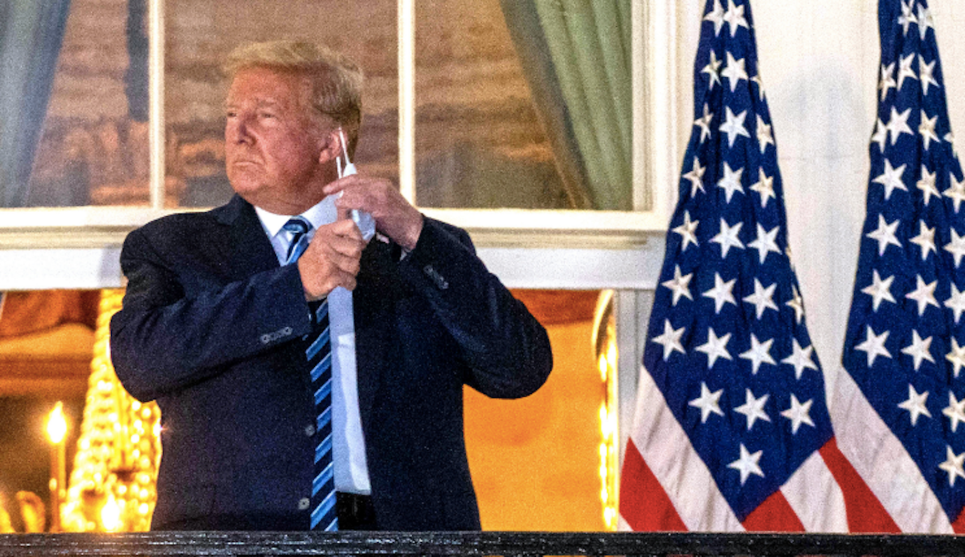
Marine One lands on the White House lawn. Donald Trump, still sick and contagious after being treated for COVID-19 at Walter Reed Medical Center, strides alone across the grass while cameras flash. Then, having climbed the steps to the balcony, he dramatically strips off his mask and salutes the helicopter as it rises toward the Washington Monument. In one of the propaganda videos of the scene uploaded to the president’s Twitter account, heroic music booms in the background—an instrumental version of a track called “Believe” from an album titled “Epic Male Songs.”
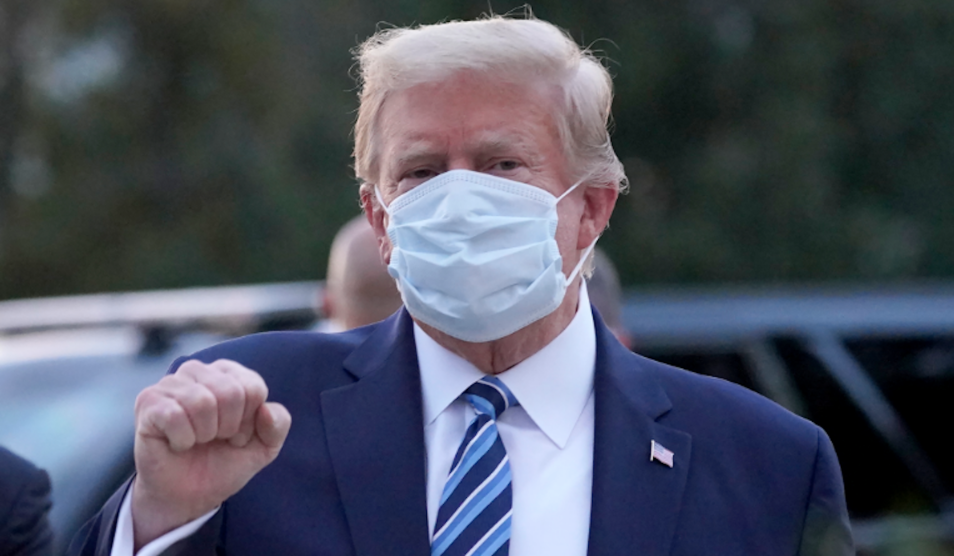
In the last few weeks, Trump and his supporters’ attempts to project masculine strength and dominance have reached literally toxic levels. “President Trump won’t have to recover from COVID. COVID will have to recover from President Trump,” Rep. Matt Gaetz (R-Fla.) tweeted. Sen. Kelly Loeffler (R-Ga.) posted an edited video of Trump wrestling the coronavirus to the ground, WWE-style. Much of the projections of the president’s manliness is tied up in the idea that he doesn’t need a mask because he is tough. “I don’t wear masks like him,” Trump said dismissively at the September 29 debate against Joe Biden. “Every time you see him, he’s got a mask. He could be speaking 200 feet away from them and he shows up with the biggest mask I’ve ever seen.” Earlier this week, he taunted House Majority Leader Nancy Pelosi by tweeting, “Wear your mask in the ‘beauty’ parlor, Nancy!”
To untangle the political and gender dynamics of Trump’s blustery response to the coronavirus and his own infection I spoke with Christina Wolbrecht, a Notre Dame political science professor who coedits the journal Politics & Gender. This spring, Wolbrecht and her colleagues put out a call for papers about COVID-19, and received multiple submissions about men and mask-wearing. Threestudiespublished in the resulting series this summer independently demonstrated links between gender identity, including sexist attitudes, and whether someone is likely to wear a mask.
Masks are a piece of cloth that you wear on your face. They protect you and the people around you. They’re not inherently a gender-related thing, but surveyshaveshown women are wearing them more often than men. What do we know about why that is?
Why do some people wear masks and others don’t? One predictor is your partisanship. We know in general that Democrats, at least up to recently, have been more likely to wear masks than Republicans. We know there’s some differences in terms of age. It turns out that another thing that explains the difference is gender identity, or the extent to which you hold sexist views. In our culture, traditional masculinity is understood as strength, vigor, and health—as not being dependent upon other people. And so to act ill, to be seen as weak, is seen as feminine. If you value masculinity, you want to move away from anything that associates you with weakness.
People who are more likely to think that women complain about things too much, and call things discrimination that aren’t, or that there should be more traditional roles in the family, are less likely to wear masks. Similarly, we see people who describe themselves as “completely masculine” and say that being masculine is very central to their sense of who they are, are less likely to wear masks. These studies suggest that the impact of having those sorts of views is bigger than, say, partisanship.
What are some qualities of masculine ideology in America that are antithetical to wearing a mask?
Public health experts have told us for a long time that men are less likely to go in for proactive doctors’ appointments, less likely to take advantage of lots of prophylactic medicines—and as a result, when they feel sick, they deny that they’re sick, go to the doctors later, et cetera—with real health consequences. This is one of the reasons why men die earlier. Public health experts for a long time have told us this is about masculinity.
It also [includes] gendered political stereotypes. There’s a long tradition in American politics and Western political development of understanding manhood—and, really, the conditions for citizenship—in these sorts of terms. You’ve got to be strong, you’ve got to be able to defend the nation, you need vigor and energy, you need to act independently. Women traditionally were understood to not have those characteristics. And that was one of the reasons they were excluded from things like the ballot box. There’s the fainting spells and the whole stereotype of women as lacking physical endurance—all associating women and illness as an opposite to masculinity.
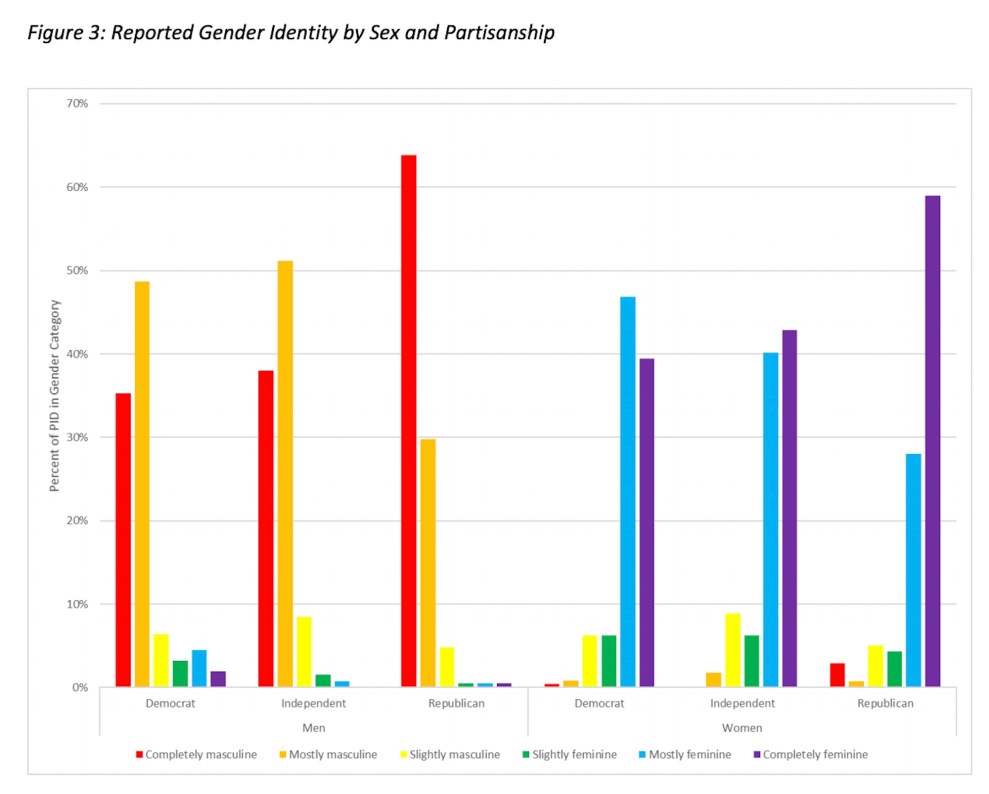
There’s also an association between people who might subscribe to more traditional masculinity and Republicanism, right? Maybe that’s my bias showing—
No! I could show you some graphs. The percentage of men in the Republican Party who describe themselves as completely masculine and say they really care about masculinity is higher than the percentage of men who say that in the Democratic Party.
One answer might be, “Oh, well, men are more likely to wear masks than women. That must be because men are more likely to be Republicans than women”—which is, in fact, true. Or you could say, “Oh, well, sexism predicts whether or not you wear a mask, but it turns out that all the sexists are Republicans and none of the Democrats are, and so really what you think is sexism is about party.” The truth is, while Democrats may be more likely to wear masks than Republicans, Democrats who hold sexist beliefs or really value being thought of as masculine are going to be less likely to do so. But a sexist Democrat still looks a bit different from the sexist Republican.
It’s like, the Venn diagram of bro-ey alpha guys, Trumpers, and non-mask wearers isn’t exactly a circle, but it’s pretty round.
That’s right.
We’ve all seen examples of “masculine” masks in pop culture—superhero movies, comics, westerns. Why are masks gendered as tough and masculine there, and as feminine in the context of this pandemic?
Nobody thinks it’s not masculine to wear a bulletproof vest, right? Protecting yourself in that way somehow means that you’re engaged in a firefight. So that’s fine, but [masks are] not. This is where the importance of framing is really important. Because it’s framed not as “You’re going off to battle, so you wear a cool bulletproof vest,” but rather, “There’s the sickness going around that makes you really tired and sniffily and may actually kill you,” [mask wearing] in some sense falls into “Real men don’t eat salads, real men don’t watch their blood pressure, real men don’t do all these things that we probably want to do if we’re trying to maintain our health.” It’s a sign of weakness.
Of course, the other piece is the cues that we’re given. Tomi Lahren, the conservative commentator, made a joke on Twitter about how Joe Biden should just get a purse to go with his mask. Being called a girl is about as unmasculine as you possibly can be. There’s been a lot of cues, especially among conservatives, as part of a broader sort of attack on the science of coronavirus. I think those messages have been pretty strong.
Especially in the White House video in which Trump, upon coming back from Walter Reed Medical Center and taking off his mask before he walks back into his workplace, announced that Americans should not let the virus “dominate” them. Is that gendered, or am I being sensitive?
Oh, my God, no. You want [to know] is this a political thing? Is this a gender thing? What I want to emphasize and say very clearly is that you cannot distinguish the two. From time immemorial, our ideas about leadership and power have been deeply gendered. That entire video, of the strong man who walks across the grass by himself, no one helps him get there, he is a leader, he goes first—that’s a very specific idea about how power is exercised. It’s not collaborative, it doesn’t take a village, it’s not in cooperation. It’s very much embodied in one person who has a very particular kind of power and strength to go up into this great, grand building, and to stand there under the lights, and the very militarized Marine One helicopter.
I don’t know if you’ve seen the more “manly” masks that are out there—the Punisher masks among them. What do they tell us about the dynamics at play here?
I would put those in the same category as the masks that match my shoes. The political theorist Judith Butler is famous for, among other things, describing gender as performative—that the way in which we present ourselves, walk, talk, dress, the accessories we wear, all of it is consciously or subconsciously a way that we express our identity. This is central to our understandings of politics as well. Partisan identities, racial identities, class identities are all things that we put on and project—and so it’s not surprising that very quickly, a market has gone grown up to provide for every possible identity you can think of. The sports identity, patriotic identity, you name it. And, in a different way but still gendered, all the RBG masks.
In the research that you’ve reviewed, is there anything about women who hold traditional beliefs about femininity and how that affects mask wearing?
The stuff on the side of women is more complicated. The effects are less consistent, and often less strong, but the same patterns hold. Preferring a traditional family, thinking that women are just out there accusing men of discrimination and unfairly trying to get an advantage—those are not views that only men hold. There are considerable swaths of the female population in the United States who hold those sorts of views as well. The research we’ve seen does suggest that women who hold what we would categorize as more sexist ideas and beliefs are less likely to wear masks, or to support mask wearing, or to support closing schools.
A lone bicyclist on a Manhattan street in August.Alex Menendez/AP
An occasional series about stuff that’s getting us through a pandemic. More here.
After the coronavirus paralyzed New York City in March, the only part of my life that became more pleasant was riding my bike.
For a moment, empty streets replaced cars parked in bike lanes, cars running red lights, cars blaring their horns for no discernible reason. On most days when I rode, I felt free. I no longer envisioned myself ensnared in the wheels of a box truck or flattened against the pavement by a charter bus that had run a red. Instead, I entertained myself, in this socially distanced reality, by riding to Rockaway Beach, or Kissena Park, or eerily silent Times Square with a clear mind.
I was still a small object amid a sea of speeding, two-ton hulls of glass and steel. But there were fewer cars overall. In April, traffic plummeted 60 percent from normal levels in Manhattan. Since then, traffic has increased, according to Politico, but was it was still down about 15 percent in August from pre-pandemic levels. That was just enough of a sustained dip for me to yearn for a reckoning.
As I biked around, I began hoping that our brief collective glimpse of a city with drastically fewer cars would convince people not to buy them at all. I hoped those who wanted to avoid crowded subways and buses would now consider opting for a (considerably less expensive) bicycle. I hoped that the outdoor dining spaces now encroaching on parking spots would remain there. And I really did hope that the island of Manhattan would set an example for other American cities by banning cars outright.
Now, I doubt that will happen. The coronavirus pandemic could have been an opportunity for New York City to dramatically shift its transportation infrastructure by taking swaths of street space away from cars and opening them up to pedestrians, cyclists, skateboarders, roller skaters, scooter riders, wheelchair users, and anyone else who scoffs at cars. But it was unequal half measures instead. After Mayor Bill de Blasio committed to blocking cars from 100 miles of the city’s streets, he reneged on his promise. Three months later, about 70 miles of roadway were closed—just over 1 percent of the city’s 6,074 miles of streets. These open streets service just 37 percent of the city’s residents, according to one estimate, and are primarily located in wealthy neighborhoods that haven’t been hit as hard by the coronavirus as lower-income communities.
I enjoyed the semi-carless city while it lasted. On long rides, I slipped the bandanna I use as a face mask down around my neck and smelled the heavy summer air. When I biked into Manhattan over the Williamsburg Bridge, I would climb about two thirds of a mile of unrelenting uphill on a narrow, graffitied bike path, dodging the cyclists who whipped by in the opposite direction. Then the skyline would rise into view as the bridge span leveled out above the East River, and the people who dotted the riverside park below appeared from this height like miniature dolls. There was no need for pedaling on the glorious decline. While cars stood still on the roadway below, gravity pulled me down the bridge into the Lower East Side’s deep embrace. Then a car horn would shatter my reverie, and I’d be back to the world I knew.
Stephen Miller, the extremist anti-immigrant Trump adviser who has promoted white nationalist ideas, lost a relative to the coronavirus pandemic, and his uncle tells Mother Jones that the Trump administration is partly to blame for this death.
On July 4, David Glosser, the brother of Miller’s mother, posted a Facebook note announcing the death of his mother, Ruth Glosser, who was Miller’s maternal grandmother:
This morning my mother, Ruth Glosser, died of the late effects of COVID-19 like so many thousands of other people; both young and old. She survived the acute infection but was left with lung and neurological damage that destroyed her will to eat and her ability to breathe well enough to sustain arousal and consciousness. Over an 8-week period she gradually slipped away and died peacefully this morning.
David Glosser is a retired neuropsychologist and passionate Trump critic who has publicly decried Miller for his anti-immigrant policies, and he contends that Trump’s initial “lack of a response” to the coronavirus crisis led to the deaths of tens of thousands of Americans who might have otherwise survived. In an interview, he says, “With the death of my mother, I’m angry and outraged at [Miller] directly and the administration he has devoted his energy to supporting.”
“Today, I tested positive for COVID-19 and am in quarantine,” Miller said in a statement.
A lot of things that have happened over the last four years could have been avoided if someone in the Trump administration had gone to theater camp as a kid or minored in dramatic theory in college.
Shortly after returning to the White House on Monday after a three-day stay at Walter Reed Medical Center, President Trump ditched his mask and filmed a 90-second campaign-style video telling us the coronavirus, which has sickened tens of millions worldwide is actually no big deal: “I learned so much about coronavirus,” the president said. “And one thing that’s for certain, don’t let it dominate you. Don’t be afraid of it.”
He added, “We have the best medicines in the world” and “the vaccines are coming momentarily.”
In essence, his message to the American people is, don’t worry about the coronavirus—go on with your lives!—because our “miracle” medicines will protect you. He is even now fundraising off this message, my colleague Abigail Weinberg reports.
But the truth is, there are no FDA-approved treatments specifically for COVID-19. A few therapies have been granted “emergency use authorizations” for hospitalized patients, and while the research behind them is encouraging, these drugs and others are far from being the medical wonders Trump is trying to sell.
The president’s COVID infomercial, therefore, is a distraction from the bigger picture: Trump’sfailure to act is killing Americans. As Mother Jones has chronicled in detail, Trump has repeatedly:
Failed to acknowledge or mourn the staggering loss of life during the pandemic (“It is what it is“)
His recent comments are simply an extension of that message. Like the pandemic, Trump’s sickness was something that would, in his reality, disappear with little explanation: “Two days ago, I felt great. Like, better…than 20 years ago,” he said, thanks to therapeutics that are like “miracles coming down from God.”
But even before his diagnosis, unproven treatments have always been the president’s answer to the pandemic: First, it was malaria drug hydroxychloroquine, then convalescent plasma, and, now, promises of a vaccine. (Though, as my colleague Kiera Butler writes, even a vaccine is unlikely to be a “silver bullet”: “Rather, it will be one more weapon against the disease to add to our arsenal.”)
Worse, his VIP treatment plan, including a buffet of cutting-edge experimental therapies, is something that’s unavailable to nearly every other COVID-19 patient. One of those therapies, for instance, is Regeneron’s lab-grown antibody “cocktail,” which has shown promising results in an analysis of 275 patients, but hasn’t yet received emergency use authorization from the FDA to treat COVID-19. According to the Washington Post, it has been administered to fewer than 10 people outside of a clinical trial. On top of that, as the Post points out, the president traveled about nine miles from the White House to his private hospital suite via helicopter, where an entire team of doctors looked after him. And even now, convalescing at “home,” he has access to unparalleled care.
Other medicines on Trump’s treatment plan reportedly include the antiviral drug remdesivir and the steroid dexamethasone—both of which are more accessible (though in the case of remdesivir, “supplies are limited,” according to the National Institutes of Health), and have large randomized controlled trials to back them up. The president has also reportedly taken famotidine, an antacid typically used to treat heartburn, Vitamin D, and Zinc, all of which are unproven COVID-19 therapies, though it’s unclear if these medications are part of his ongoing treatment.
“This is the President of the USA. He is going to get the kitchen sink thrown at him medically, offered all there is—whether it’s authorized under emergency use or not, in the case of the antibody treatment,” epidemiologist Dr. Seema Yasmin told CNN. “But then there are (almost) 210,000 Americans who have died over the past few months because the pandemic response has been so bad. And they certainly didn’t get access to this kind of treatment.”
This isn’t just a bad look. It’s shoddily crafted fiction. Donald Trump basically told the rest of us—who do not have access to the world’s top-tier medical resources—that we have nothing to fear from this virus because “you’re gonna beat it.” Clearly, not everyone beats COVID, and the president saying so is reckless. It’s sort of like telling people in the midst of a climate crisis to not worry because “there is plenty of great housing away from the coasts!”
Trump had an opportunity to show real compassion and empathy for the other patients who have developed COVID-19, and, perhaps, to urge Americans to abide by the key recommendations that have been proven to actually work, and are inexpensive and widely available: social distancing and mask wearing. Instead, he basically suggested that the 210,000 people who have died in this country from the coronavirus did so because they weren’t…tough enough?
Medical experts have already pointed out how careless this idea is. “Are you kidding me?” tweeted UC-San Francisco department of medicine chair Dr. Robert Wachter. “After 210,000 deaths in the U.S. & 1 million deaths worldwide? This either shows a breathtakingly callous, inhumane & counterproductive attitude, or he has altered mental status.” Harald Schmidt, an assistant professor of medical ethics and health policy at the University of Pennsylvania told the New York Times, “I am struggling for words—this is crazy. It is just utterly irresponsible.”
Nevermind the rallies and Rose Garden ceremonies and donor events Trump held, or his insisting that people around him don’t wear masks or conduct contact tracing: If you ask the president, contracting the coronavirus is a symbol of leadership, not a lack of it. In a rambling portion of his video update, the president, sounding very much like someone who had just ingested a concoction of drugs, said, “We’re going back—we’re going back to work. We’re going to be out front. As your leader, I had to do that. I knew there’s danger to it, but I had to do it. I stood out front. I led. Nobody that’s a leader would not do what I did. And I know there’s a risk, there’s a danger, but that’s okay—and now I’m better, and maybe I’m immune! I don’t know.”
For now, we’ll have to wait and see if this backfires politically—and even, perhaps, medically. Aside from the known side effects of these drugs, doctors, including the president’s own physician Dr. Sean Conley, acknowledge that it’s uncertain what effect mixing them all together will have. “We’re in a bit of uncharted territory when it comes to a patient that received the therapies he has so early in the course,” Conley said during a briefing with reporters Monday.
But, Conley added, “[He has] 24/7 world-class medical care surrounding him down there. We’re not going to miss anything.”
Admiral Charles Ray, the vice commandant of the Coast Guard, tested positive for COVID-19 and will have to quarantine at home, the Coast Guard announced Monday.
Ray, who is the second-highest-ranking military official in the Coast Guard, tested positive on Monday “after feeling mild symptoms over the weekend,” a spokesperson said. It is not clear if his diagnosis was related to the apparent super-spreader event at the White House on Saturday, September 26, which was held to honor Supreme Court nominee Amy Coney Barrett. At least 11 attendees, including President Donald Trump, have since tested positive for the coronavirus, but the White House has declined to conduct contact tracing that would help establish the source of the infections. Ray was at the White House a day after the Barrett event. He “began feeling unwell” on Friday, October 2, and eventually tested positive three days later, according to Fox News’ Jennifer Griffin.
Ray’s diagnosis has already had a sprawling impact on the military. Several senior officials were in close contact with Ray, including Gen. Mark Milley, chair of the Joint Chiefs of Staff, and they are now quarantining, CNN reported.
More military leaders could be affected. After news of Ray’s diagnosis broke Tuesday afternoon, Pentagon spokesperson Jonathan Hoffman said Ray was in meetings with “other Service Chiefs” at the Pentagon last week. “Out of abundance of caution, all potential close contacts from these meetings are self-quarantining and have been tested this morning,” Hoffman said. “No Pentagon contacts have exhibited symptoms and we have no additional positive tests to report at this time.”
Already some of the names of Ray’s contacts have trickled out:
BREAKING: CBS News reports top U.S. military officials quarantined after COVID19 exposure: Chairman of Joint Chiefs of Staff Vice Chairman Army chief of staff Naval Operations Chief Air Force chief of staff CyberCom Commander SpaceForce operations chief (@davidmartinmep reports)
The United States faces a presidential election in less than a month, and its two highest-ranking military officers—not to mention the commander-in-chief himself—are in quarantine.
President Donald Trump, clearly unchastened by his hospitalization for COVID-19, is back to comparing the virus to the flu. It’s the same, tired falsehood he’s clung to—at least publicly—since the start of the pandemic, as he seeks to downplay the deadly disease, discourage public health interventions, and project strength amid an increasingly imperiled reelection campaign. Except this time, Trump significantly escalated the death toll from the flu, falsely claiming that it is more lethal than the coronavirus in “most populations.”
Take a look at Tuesday’s tweet and one he fired off in March:
Flu season is coming up! Many people every year, sometimes over 100,000, and despite the Vaccine, die from the Flu. Are we going to close down our Country? No, we have learned to live with it, just like we are learning to live with Covid, in most populations far less lethal!!!
So last year 37,000 Americans died from the common Flu. It averages between 27,000 and 70,000 per year. Nothing is shut down, life & the economy go on. At this moment there are 546 confirmed cases of CoronaVirus, with 22 deaths. Think about that!
So, what’s changed between March and today? More than 200,000 deaths in the United States, an economic crisis, a White House outbreak that continues to unfold, and a newly infected president. The mortality rate from the flu, however, has not. According to data from the Centers for Disease Control and Prevention, the estimated range of annual flu deaths in the United States over the past decade has been 12,000 to 61,000—well below Trump’s new figure of more than 100,000 people. What’s more, this isn’t even a straight comparison. The more than 200,000 deaths from COVID-19 have come despite widespread shutdowns, mask mandates, and social distancing campaigns—without these unprecedented measures, the death toll would presumably be far higher.
Trump actually knows all this. Back in February, he privately acknowledged to journalist Bod Woodward that COVID is “more deadly than even your strenuous flus.”A month later, Trump told Woodward, “I wanted to always play it down. I still like playing it down, because I don’t want to create a panic.”
Trump’s latest entry into his coronavirus denial comes a day after returned to the White House from Walter Reed Medical Center still contagious with the virus, defying public health guidance. “Don’t be afraid of COVID,” he tweeted. “Don’t let it dominate your life.”
In the early hours of Friday morning, the White House announced that President Trump and his wife, Melania, had tested positive for the coronavirus. Almost immediately, there were calls for expressions of empathy for them as they were diagnosed with this potentially deadly disease that has already killed 207,000 people.
Interesting to see those who’ve spent the last few years screaming that Trump’s an uncaring, heartless empathy-devoid b*stard now spewing their gleeful joy that he & his wife have a deadly virus. They’re no better than the man they loathe.
Former Vice President and Democratic presidential hopeful Joe Biden immediately sent out his best wishes to the couple.
Jill and I send our thoughts to President Trump and First Lady Melania Trump for a swift recovery. We will continue to pray for the health and safety of the president and his family.
In the past, presidents have served as role models, the consolers-in-chief during times of national tragedy. One need only look at Ronald Reagan during the Challenger disaster, Bill Clinton after the Oklahoma City bombing, George W. Bush after 9/11, and Barack Obama after the mass shooting in Newtown and the racist murders in the Black church in Charleston, to see presidential eloquence in expressing grief for the nation. But from the very beginning of his presidency, Trump has chosen not to occupy that role—culminating in his responses to the pandemic.
When the coronavirus began to spread in the United States, Trump immediately began to downplay its seriousness—even as he admitted to journalist Bob Woodward that he appreciated COVID-19 was far deadlier than the flu. As the death toll climbed, Trump not only did not implement an effective systemic public health response but refused to acknowledge the collective grief bearing down on a nation. As families and communities struggled to mourn over Zoom and suffered through the loss of physical contact with loved ones, the president pressured everyone to just get on with their lives.
To make matters worse, his inability to understand science has led to what is considered to be one of the worst pandemic responses in the world, leading to unnecessary loss of life. Trump has flip-flopped on mask-wearing, sometimes saying he’s fine with masks but also mocking Biden for wearing a mask in public and demeaning the size of Biden’s socially-distant campaign events. Trump has insisted that the virus would disappear without a vaccine but is also bragging about how a vaccine will be ready in a matter of weeks. His blatant contradictions of his own public health officials have resulted in mass confusion. Beyond the cacophony of misleading statements and outright lies, one thing has remained constant: Trump doesn’t care about coronavirus victims.
But now he’s one of them. After months of traveling to crowded rallies without a mask, Trump and the First Lady—not to mention members of his closest staff— have joined the more than 7 million people in the US who have contracted COVID-19. According to the White House, the president is experiencing “mild symptoms” of the virus.
The level of sheer heartlessness coming from the White House is difficult to overstate. In August, when the death toll was at 158,000, Axios reporter Jonathan Swan asked Trump about the staggering death toll. “It is what it is,” Trump responded, with some irritation. When the United States crossed the grim milestone of 200,000 late last month. Trump offered no sympathy or condolence, instead opting for more of the denial that’s characterized his pandemic response. “This affects virtually nobody,” he told thousands of people at a packed rally in Minnesota. “Nobody” for Trump equals hundreds and thousands people, a disproportionate amount of them who are Black and Brown and poor.
Of course, the signs that empathy would simply not be in the cards for this presidency were obvious from the beginning. In the early days of his campaign, he mocked Serge Kovaleski, a reporter with a disability that makes it difficult to move his arms. Then, in the weeks leading up to the 2016 election, Hillary Clinton contracted pneumonia and was caught on tape falling down. Trump ridiculed her at a rally and pretended to stumble on stage.
In 2017, after Hurricane Maria brought catastrophic winds and rains to Puerto Rico, leaving millions without water, food, or electricity, Trump chose to spar with San Juan’s mayor Carmen Yulín Cruz, blaming her for the disaster. When he finally went to the island, he tossed paper towel rolls into the crowd. The First Lady is not exempt. In 2018, on a trip to Texas where the administration was holding children who had been separated from their parents at the border, Melania was photographed boarding a plane in a green jacket that said, “I Really Don’t Care. Do U?”
Underpinning the disastrous response to the pandemic has been the ongoing plague of racism in the United States and the attempted reckoning for racial justice. When George Floyd, a 46-year-old Black man in Minneapolis, was killed by a white police officer who knelt on his neck for nearly nine minutes, Trump tried to offer words of support for Floyd’s family—but could never quite get there. It wasn’t long before the president was retweeting pundits impugning Floyd’s character and threatening to shoot Black Lives Matter protesters. He did not hesitate, however, to offer words of support for Kyle Rittenhouse, the white 17-year-old charged with murder after he killed two racial justice protesters. The message was clear: The president does not care about Black lives—or the people who do.
During the first memorably chaotic presidential debate two days before the president revealed his diagnosis, Trump brought his lack of empathy to new lows. When Joe Biden referred to the impressive military service of his late son, Beau, who died of brain cancer in 2015, Trump taunted his opponent. “Are you talking about Hunter?” he asked, knowing the answer. “No, I’m talking about Beau,” Biden replied. “I don’t know Beau,” Trump shot back and then attempted to focus on Hunter Biden’s ties to Ukraine. At that same debate, Trump refused to denounce the Proud Boys, a neo-fascist group. Two days later, he got COVID.
The defenders of civility may think that the only appropriate response from liberals, Democrats, and the American public in general is empathy for the First Family as they face this health crisis. But Trump has not bothered with even the most pro forma expression of sympathy or sadness for coronavirus victims. And for Black and Brown people and other marginalized groups, he’s expressed actual disdain. He’s an incompetent racist who only cares about his own fundraising and reelection; his aversion to sympathy has led to the highest coronavirus death toll in the world and an alarming uptick in white supremacist violence and rhetoric. To demand empathy in the face of such deadly indifference is not civility at all—it just adds to the cruelty.
President Donald Trump introduces Judge Amy Coney Barrett as his nominee to the US Supreme Court on September 26, 2020 in the Rose Garden at the White House.Gripas Yuri/POOL via ZUMA
Mitch McConnell has the votes to confirm Amy Coney Barrett to the Supreme Court before November 3. Fellow Republicans are excited to cement a conservative 6–3 majority on the nation’s highest court. Democrats had struggled to figure out how to impede the rush to confirmation, but there was always one thing that could get in the way, and it appears to be working its way through the ranks of his party: the coronavirus.
By early Friday afternoon, it has become clear that not only have President Donald Trump, his wife, and top aide Hope Hicks contracted the virus, but so has Sen. Mike Lee (R-Utah). Lee attended the ceremony announcing Barrett’s nomination last Saturday, then proceeded throughout the week to attend multiple meetings on Capitol Hill, including a Thursday hearing with the Senate Judiciary Committee. Lee is a member, and it’s that committee that is slated to hold Barrett’s confirmation hearing in just 10 days. It will take a few days to learn if Lee infected any of his colleagues. Lee, who said he had allergy-like symptoms, is claiming he will emerge from his quarantine just in time for Barrett’s hearing.
Already, a battle is brewing over whether to delay the hearing due to the spread of the virus. The committee’s ranking Democrat, California’s Dianne Feinstein, put out the first shot on Friday, urging chair Lindsey Graham (R-SC) to, in the event of a needed quarantine, postpone the hearings rather than push ahead with a virtual confirmation. “It’s critical that Chairman Graham put the health of senators, the nominee, and staff first—and ensure a full and fair hearing that is not rushed, not truncated, and not virtual,” Feinstein said in a statement. “Otherwise this already illegitimate process will become a dangerous one.”
Early reporting on Capitol Hill reveals Republicans are also panicking about the prospect of Barrett’s confirmation being delayed by COVID.
A Senate GOP aide, on background, tells the Post that some Rs are now discussing asking Leader McConnell to "take the Senate out of session next week" before the ACB hearings start in mid-October.
"If some in the Republican caucus get sick, we are screwed," the aide says.
While McConnell currently has the votes to confirm Barrett, he doesn’t have many to spare. Graham could plow ahead with a virtual hearing for Barrett, a move that could further erode public trust in the Senate and the Supreme Court. But in hindsight, the situation suggests that McConnell and House Speaker Nancy Pelosi should not have declined to institute rapid testing protocols on Capitol Hill. This story of a wave in Congress is likely just beginning: on Friday, CNN reporters said that Republican members of Congress who had been on Air Force One with the president were walking and voting on the House floor without taking any noticeable precautions to protect their fellow lawmakers.
For months, the biggest threat to Trump and McConnell’s prospects of remaining in power and furthering their agenda has been the coronavirus. Their inability and refusal to protect the country or offer relief already put them on the ropes. Now their decisions to sacrifice their own safety on the altar of Trump’s scientific denialism threatens to land another blow.
Anonymous As Told To Kiera ButlerSeptember 29, 2020
Mother Jones Illustration
We asked people who have quit since January 2020 how and why they did it. You can read more about the project, and the initial nine stories, here. Got your own quitting tale? Send us an email.
Anonymous, 62
Position: Tenured professor, University of West Georgia Started: Late 1990s Quit: Summer 2020 Salary: Prefer not to say
As told to Kiera Butler
I felt that the handling of things last March was quite sane. When they announced that spring break would be extended by one week to give professors time to reorient their classes to an online format, I thought, “Bravo. That’s really good.”
But then on May 11, we had a communication that made it clear that there would be an on-campus instructional presence in the fall, with accommodations for faculty and students as needed. So I’m thinking, “Wow, it’s so far from the fall, and they’re already telling us there’s a commitment to on-campus presence.” Now, knowing that I’m in the state of Georgia, knowing that the chancellor of the university system of Georgia is appointed by the governor, I was immediately very uncomfortable about what the future portended. I felt that there was not going to be a sane response to the pandemic in the fall. And that there would be some sort of allegiance to an economic priority. I think that turned out to be the case.
There was a lot of communication from the new president who had started in April. He was basically saying: We’re going to follow the science, we’re going to follow the CDC, and we’re going to follow the governor’s office. Then, at some point, there was kind of an odd video message. He announced that we were going to open in the fall, and he was sort of cheering. I’m thinking, “Oh great, you’re going to kill people, yay.”
I was very unhappy about it. At that point, they had already intimated that there might be an early retirement opportunity. There was also a suggestion that we would be able to opt out of teaching face-to-face, that we could do everything online. I didn’t know if they would ultimately offer the retirement incentive. In fact, when it did come out, there was a disclaimer that there was no guarantee you’re going to get it if you apply for it. I was very interested in the teaching online option, so I pursued that.
Someone in Human Resources told me that the university system in Georgia would allow accommodations to faculty and staff who themselves have a high-risk designation. But not if you have family members with a high-risk designation. The human resources person said that even though that’s the policy, the University of West Georgia will try to accommodate people who have family members who are high-risk designation. So I went ahead because my spouse is in that category.
A few days later, I got a phone call from HR asking me about the accommodation. I explained again about my spouse’s situation. And then—this was a little surreal—not five minutes later, I got an email from the same person. It was a form message telling me, “we received your request for this accommodation, sorry to tell you that we’re not able to fulfill it.” I was like, why did they even call me? It was very strange. And the letter says something to the effect that it’s because we have too many requests. I know people who are in the same situation I was in: They were denied.
I felt anxious. I thought, “What if I don’t get the retirement?” I’m imagining if I have to teach, I’m going to need to make some kind of alternative living arrangement, so that my spouse is not exposed. And that was my major concern. I really was feeling like, if my spouse gets COVID, I don’t know that they would survive. This is a scary thing. I talked to a different person HR who encouraged me to seek an exemption for myself. So I actually did have a tele-session with my doctor. I explained the situation to him, and he wrote a very general note about me. I resubmitted a form for myself, and it was approved.
So, I breathed a sigh of relief that I would not have to teach in the classroom. But my colleagues who didn’t have an accommodation to teach online were told they me had to design their classes both online and face-to-face, in what they called a “dual modality, delivery mode.” What that really means was so vague, and it was always changing. It was crazy. Sometimes they would contradict the thing they just said the week before. There was a meeting where the provost said something to the effect that if you have a graduate class, and all the graduate students want to meet online, they can. But then a few days later, he came back with an email saying it had to be face-to-face. And then they started making it hard for students to opt-out of face-to-face classes. What I found so absurd about the situation is that we have never, in my time at the university, been required to have an attendance policy that requires students to come to class. But now we do.
All of this creates a tremendous burden on all the professors who themselves are having to deal with this pandemic in their own personal lives—and without any compensation for doing that. Several years before the pandemic, the University of West Georgia was developing its online learning capacities. They were offering professors $5,000 to train over the summer—to have formal training on how to teach online. (Editor’s note: The university disputes this claim. “UWG is not aware of recent institutional incentive programs for online instruction,” a spokesperson said. But another faculty member reached out to Mother Jones after the publication of the article to confirm that instructors “did receive [financial] incentives for training in online instruction over the summer.”) And now you’ve got people who’ve never taught online or very rarely taught online who are just thrown into it. It’s a tremendous amount of work.
I realized I could teach for another couple of years, but not in a way that is fulfilling to me. Even though I had the online teaching accommodation this semester, I was still employed by the university, and I didn’t know what awkward or uncomfortable situation I was going to find myself in eventually. It really felt to me like I was now operating under an authoritarian sensibility. This whole idea of faculty governance—we’ve seen such an erosion of it. It used to be, former presidents would consult faculty to get their input on things. But the new president—it’s like he doesn’t even understand the concept of faculty governance. He was asked in a virtual town hall, “How many faculty did you consult in this reorganization? And how many will you consult moving forward is as plans unfold?” His response was basically, I won’t tell you how to do your job and you don’t tell me how to do my job. (Editor’s note: A spokesperson for the university said this characterization “is not correct” and that the president seeks input from faculty. “We have depended on the input of hundreds of faculty and staff members to research, develop, and implement our plans,” a spokesperson said. But the UWG chapter of the American Association of University Professors backed up the retired professor, saying the university has “not consulted with faculty about any of the COVID-related decisions that have been made.” A faculty member also reached out separately to dispute the university’s claim, in an email. “I can confirm firsthand that faculty were not consulted in the reorganization [of my department],” they wrote.)
It is true that the administration had to deal with a massive reduction in the budget. And when they announced initially that they were managing to do this without firing anybody or letting any of the faculty go, I was very happy. I felt wonderful. What I didn’t realize was that they were going to balance the budget by gutting the traditional arts and sciences disciplines. The business school curriculum was unaffected. Education was unaffected. But the traditional arts and sciences—history and science and the social sciences, all of those types of disciplines—were to be massively reorganized, and 17 departments would be reduced to four. There’s been this proliferation of administrative personnel—so many assistant deans and associate deans and so forth—and instead of making cuts there, which would have saved big money, they predominantly cut chairs as opposed to higher-level administrative positions.
The administration is saying they’ve done this reorganization in such a way that it will not impact the students at all. They’re not losing any courses or degree programs. And that’s true. But they do lose the intangible advantages that come from having a departmental identity. There’s a loss of community and cohesion. Also, some of our staff are gone. They’ve lost their jobs—people who are extremely hard-working, wonderful, helpful, dedicated workers, and now they’re gone. They took with them a lot of administrative skill and person hours to put into administrative tasks that now the faculty themselves have to do. So another intangible loss for the students will be that they’ll have less of the time and energy and focus and research from the faculty.
I do feel sad about leaving, but the damage was already done whether I left or not. I feel gratitude that I am in the position that I can be outside of that situation and I can refashion the rest of my life. I’m very excited about that.
But when I think of my colleagues, I just feel bad for those who have to negotiate going into the classroom. The word “terrified”—I’ve heard that word used so many times by people who have to teach in person. They’ll say, “I’m terrified.”
*This article has been updated to include a statement from the chapter of the American Association of University Professors at UWG and a statement from another faculty member who read the initial piece.
My house has a strict quarantine policy. I share indoor space with my fiveroommates and a few others in our pod, and only see most friends outdoors, 6 feet away and/or wearing masks. Yet whenever someone we know is passing through town, we end up voting to let them spend the night or even a week, sharing our kitchen, bathroom, and germs. This feels safe because our friends are also quarantining. Like us, they work remotely, can easily get tested, and have little issue receiving public health guidance.
If I weren’t working in media and wearing a mask in public (and feeling occasionally deprived of my favorite social pastimes—concerts and festivals), I could probably forget there’s a global pandemic going on. I never lost my job, many of my peers have resumed flying, and nobody I know has gotten sick since April. Instead, we’re taking advantage of remote-work policies to bounce between AirBNBs in sunny locales, with more time to self-reflect and connect with family. I’m so confident in my negative COVID status that I even stayed over at my grandparents’ house last month. The whole thing’s started to feel like a surreal collective vacation.
Some are even more removed, able to afford Zoom tutors and in-home teachers so their kids’ schooling doesn’t miss a beat. $500 rapid tests—“the new velvet rope”—allow the 1 percent to gather risk-free, merging their pods into a caste-based bubble where the virus doesn’t exist. “Have they been quarantining?” we ask when deciding if someone’s safe for our roommate to kiss. The subtext is, “can they afford to?”; if not, they can’t come to our party.
COVID-19 kills: as of this week, 200,000 people in our country alone. Barring a miracle vaccine before winter, the worst may be still yet to come. In California, where I live, August was the deadliest month of the entire pandemic, with 3,745 lives lost, an 18 percent increase over July. The brunt of this mass death is being borne by Black, Latino, and Indigenous people, particularly those in income brackets lower than my own, where economic necessity forces many to keep packing meat, delivering groceries, dropping off takeout, and cleaning hotels for the rest of us. Our bubble rests on their backs, is kept inflated by the same lungs that coronavirus attacks. None of this is news, but six months into the pandemic, the numbers keep getting worse.
Thanks to institutional racism in American science and medicine, we’ve only slowly glimpsed a full picture of COVID-19’s disparities. By May, it was clear that the states who rushed to re-open saw the most unequal share of Black death. In July, we knew that seven Indigenous tribes had case rates higher than that of any US state. And by September, what had three months prior been a 35 point gap in white and Black mortality rates swelled to 51, according to Andi Egbert of the APM Research Lab. The gap between white and Indigenous grew from 10 to 35, while the over-representation of Latino and Pacific Islander deaths continued to expand as well. When you adjust by age, the disparities get even worse. Today, white people are dying from COVID-19 at lower rates than Black people die without it.
Yes, the pandemic is merely exacerbating disparities that already existed. As disease historian Frank M. Snowden told the New Yorker, diseases spread “along the fault lines created by poverty and inequality.” Black people already had asthma and lung disease; Latinos worked jobs that didn’t offer healthcare; Indigenous communities lacked information access and mistrusted Western institutions. Sometimes I hear myself and other white folks regurgitate these lines with an air of resignation, as if the situation is inevitable, absolving us of guilt. If this is just the way things are, then it’s tragic, but there’s not much we can do. In fact, our inaction is ushering in a new era of deadly American racism: some of us stay afloat or even rise, while others sink and maybe drown. COVID begets more racialized poverty begets more COVID, ad nauseum.
Before the pandemic started, American billionaires collectively held about $3 trillion. In the last six months, as most people dreaded an economic depression, the billionaires grew their hoard by nearly a third, $845 billion and counting. It’s never been more blatant or painful to see: profits are the unpaid wages of the working class.
My upper-class white peers and I were already insulated from the suffering of Black, Brown, and working-class communities, but under COVID, the distance has increased. We’ve fled cities to seek the open space and fresh air of the countryside and suburbs, while also closing ourselves off to friends, lovers, and relatives who don’t meet our safety standards. Both geographically and socially removed, we’re less likely to feel the pressing need to take action. We see the numbers but they don’t affect us; we no longer have to hear the sirens. Besides a grandparent here and there, the dead are not people we know.
The same is likely true for our national leaders, whose procrastination in passing a second aid package has left Americans to bail each other out. But even that urgency has faded: In the early days of the pandemic, my friends launched a mutual aid effort inviting still-employed workers to make direct cash payments to people who’d lost their jobs. $100,000 was moved in a matter of days. Then payments slowed to a crawl, with just $73,000 donated over the next five months. This summer, I helped them make a last-ditch appeal to people who’ve been working remotely, asking them to consider sending what they used to spend on their commute as a weekly donation to a Black or Brown person in need.
Perhaps, as the threat of infection has begun to feel farther away, mutual aid has fallen out of vogue. Of the 27,000 who saw our Instagram ad, only one person signed up to give.
Sen. Rand Paul (R-Ky.) suggested at Wednesday’s Senate hearing on the federal pandemic response that shutdowns did not curb the spread of the coronavirus. Dr. Anthony Fauci wasn’t having it.
“You’ve lauded New York for their policy,” Paul said during the Health, Education, Labor and Pensions subcommittee hearing. “New York had the highest death rate in the world. How can we possibly be jumping up and down and saying, ‘Oh, Governor Cuomo did a great job’?”
“No, you misconstrued that, senator, and you’ve done that repetitively in the past,” Fauci replied. “They got hit very badly, they made some mistakes. Right now, if you look at what’s going on right now, the things that are going on in New York, to get their test positivity to 1 percent or less, is because they are looking at the guidelines that we have put together from the task force of the four or five things, or masks, social distancing, outdoors more than indoors, avoiding crowds, and washing hands.”
“Or they have developed enough community immunity that they’re no longer having the pandemic because they have enough immunity in New York City to actually stop it,” Paul interjected.
“This happens with Senator Rand all the time,” Fauci said. “You were not listening to what the director of the CDC said, that in New York it’s about 22 percent. If you believe that 22 percent is herd immunity, I believe you’re alone in that.”
Watch the video:
FAUCI to Sen. Paul: "You are not listening … If you believe that 22% is 'herd immunity', I believe you're alone in that."pic.twitter.com/WykoaZwRT3
The United States has passed the milestone of 200,000 coronavirus deaths and the number is still climbing. Since the pandemic began, President Donald Trump has lied about the virus, downplayed its severity, and (in an impressive feat of scientific ignorance even for him) discouraged his followers and sycophants from wearing masks—even as his appointee to the CDC testified that absent a vaccine, a mask is the best way to protect yourself and everyone around you. But as the pandemic wears on and the election creeps closer, Trump—who has spent the last six months ignoring public health officials, when he’s not undermining and attacking them—is now using the possibility of a vaccine as a cynical election ploy.
Suddenly, the country’s science-denier-in-chief was making claims that a vaccine would be ready just in time for his re-election. “It will be delivered before the end of the year, in my opinion, before the end of the year,” Trump said at a rally in Pennsylvania earlier this month. “It really might even be delivered before the end of October.” From the outset, experts have warned that even though efforts are underway to create a COVID-19 vaccine at record speed, it would still take about 18 months to develop and test one, and then still more time to distribute doses around the country. Critics of the president, including his Democratic opponent, recognized the absurdity of the situation immediately.
“I trust vaccines, I trust scientists, but I don’t trust Donald Trump,” former Vice President and Democratic presidential nominee Joe Biden said last week. Trump’s response, since acknowledging science and the reality of the dire public health crisis is simply out of the question, turned valid criticism of him into a disingenuous smear: Biden, Trump announced, is an anti-vaxxer.
President Trump says "Joe Biden's anti-vaccine theories are putting a lot of lives at risk." pic.twitter.com/Mb5ybudHH8
“They’re only doing it for political reasons, it’s very foolish.” Trump said at a White House briefing last week. “It’s part of their war to try and discredit the vaccine now that they know that we essentially have it.” The pattern of deploying multiple lies—there is no vaccine, Biden is not anti-science—is an attempt to disguise a larger truth: The president doesn’t know to attack his opponent.
Trump has played footsies with anti-vaxxers for years and endorsed the discredited idea that vaccines can cause autism in children. “Ithink the vaccines can be very dangerous,” he said during the 2009 swine flu pandemic. “And, obviously, you know, a lot of people are talking about vaccines with children with respect to autism.” Now, he wishes to declare that being anti-vaxx is bad and it was Biden who believed it all along. After all, for Trump, the vaccine was never about a responsible response to the pandemic, but a convenient talking point for his campaign.
For those keeping score at home, not only does Trump continue to insist that the virus will just magically disappear one day, he also suggested injecting bleach as a way to cure coronavirus, and pushed hydroxychloroquine, an anti-malarial drug, despite studies showing that it could be dangerous. The whiplash was almost painful. First Trump started telling the public that a vaccine would be available before election day. Then he insisted at a rally on Monday, “This virus affects virtually nobody.”
“The virus affects virtually nobody. It’s an amazing thing.”
Just curious, if the virus isn’t even that serious and would simply vanish, why does a vaccine need to be pushed out in record speeds? And if COVID “affects virtually nobody,” what about the 200,000 people who died?
The answer is simple. The president has been playing politics with the coronavirus all year. When the CDC attempted to warn the public about how severe the problem would be, Trump went apocalyptic, even though he knew the virus was far deadlier and more contagious than the flu, as revealed in a series of interviews he conducted with journalist and author Bob Woodward. Since then, the Trump administration has silenced its own government officials, meddled in the science, and created mass confusion.
Last week at a congressional hearing, Centers for Disease Control director Robert Redfield said masks may protect us more than a vaccine (because your immune system may not respond to the vaccine), and that a vaccine wouldn’t be available to the public until next summer or fall. Later that day, Trump said his CDC director was wrong about masks and the speed at which a vaccine would be available. “It’s just incorrect information,” Trump said. “When he said it, I believe he was confused.” And if that wasn’t enough to make it seem like the politicization of a coronavirus vaccine, the New York Times reported that Alex Azar, the head of the Department of Health and Human Services has barred the Food and Drug Administration from signing new rules about food, medicines, and vaccines. It’s unclear what that means for a possible COVID-19 vaccine, but Dr. Peter Lurie, a former associate commissioner of the FDA, described the move as “a power grab.”
One of the many bleak aspects about the pandemic is that Trump has chosen to focus on vaccines, which may or may not work, while ridiculing the proven tools at our disposal: mask wearing and social distancing. And even while Trump’s meddling and insistence that a vaccine will be ready by the election is not helping him in the polls; it is eroding trust in government. Only 27 percent of Americans say they are confident in Trump’s judgement on a vaccine. And the latest grim milestone we’ve crossed will only make it worse.
As the death toll and the number of infected people continue to climb unabated, the response from the federal government has been dismal. There has been little in the way of economic relief, as millions face hunger and homelessness. There has been no national strategy on testing, tracing, and isolating the sick. There hasn’t even been the bare minimum: a moment of public mourning, even a ceremony, for the lives lost. After more than six months of the crisis and 200,000 families and communities irreparably broken, all Trump has to offer is inept political gaming and an illogical smear on his opponent.
And we respect that! But maybe you’re of a mind to support our work directly instead? We have until December 31 to raise the last $400,000 we need to keep our nonprofit newsroom running at full strength into 2026. Will you make a gift today?
We noticed you have an ad blocker on. Can you pitch in a few bucks to help fund Mother Jones' investigative journalism?
Billionaires own the media,
but they don’t own us.
At Mother Jones we know these aren’t conventional times, and they require unconventional coverage. That’s what deliver every day: fierce, independent journalism you can’t find elsewhere. Perhaps never in the history of our country has that been more necessary than now. But we can’t do it without reader support—your support. Please chip in today.
Billionaires own the media,
but they don’t own us.
At Mother Jones we know these aren’t conventional times, and they require unconventional coverage. That’s what deliver every day: fierce, independent journalism you can’t find elsewhere. Perhaps never in the history of our country has that been more necessary than now. But we can’t do it without reader support—your support. Please chip in today.