Another update in the hydroxychloroquine saga: The Food and Drug Administration has revoked its emergency use authorization for the controversial drug, which President Donald Trump has aggressively promoted and, at one point, claimed to be taking prophylactically.
The FDA said in its announcement that the suggested doses of chloroquine and hydroxychlorine “are unlikely to produce an antiviral effect” and that data from a recent randomized controlled trial did not show benefits over standard of care alone.
The bottom line, according to the FDA, is that “it is no longer reasonable to believe that oral formulations of HCQ and CQ may be effective in treating COVID-19, nor is it reasonable to believe that the known and potential benefits of these products outweigh their known and potential risks.”
Trump said in late May that he’d finished his two-week regimen of hydroxychloroquine—perhaps now he’ll stop urging others to take the drug.
The top public health official in Tulsa wishes Donald Trump would stay away next week. When the president recently announced he would resume his in-person arena rallies after they were put on pause because of the coronavirus pandemic, his first scheduled stop was set for the Oklahoma city on June 20. While the campaign plans to fill a 19,000-person indoor stadium there, health officials are cautioning that the rally could have deadly consequences.
“COVID is here in Tulsa, it is transmitting very efficiently,” warned Dr. Bruce Dart, director of Tulsa’s City-County Health Department, in theTulsa World. “I wish we could postpone this to a time when the virus isn’t as large a concern as it is today.” On Saturday, Oklahoma reported 225 new infections, a new daily high. As of Sunday, Oklahoma was reporting more than 8,000 infections and 359 deaths.
Dr. Dart blames the spike in infections on several factors, including quarantine fatigue, and warned that a large outbreak had the possibility of overwhelming the county’s health system. “A large indoor rally with 19-20,000 people is a huge risk factor today in Tulsa, Oklahoma,” he said before suggesting Trump could fall ill as a result of his own event. “I’m concerned about our ability to protect anyone who attends a large, indoor event, and I’m also concerned about our ability to ensure the president stays safe as well.”
“I think it’s an honor for Tulsa to have a sitting president want to come and visit our community, but not during a pandemic,” Dart added, telling the newspaper he was concerned infections touched off by travelers and crowds attending the rally could swamp local treatment capacity.
Several states that, like Oklahoma, were spared the worst in the early days of the pandemic are now recording a surge in infections and hospitalizations. On Saturday, 22 states reported increases in their daily cases. Relaxing restrictions aimed at stemming the virus’s spread have prompted health experts to warn that the country could see more outbreaks, spurred along by growing indoor gatherings.
But the president is prepared to go ahead with the rally, after rescheduling it from June 19, the day the Juneteenth holiday is celebrated marking Black people’s liberation from slavery. (Critics had pointed out the insensitivity of hosting a rally on that day, especially given the city’s history as a site of a major 20th century anti-Black massacre.)
Despite his track record of downplaying the seriousness of the disease, fumbling the federal response, and shunning masks, Trump and his campaign know they are subjecting his fans to risk by holding the rally: attendees must submit a form agreeing to not sue the campaign if they contract COVID-19.
Two distinct videos went viral over the Memorial Day weekend. One was of crowds of people partying and drinking at an Ozarks’ pool resort in Missouri. The other was of a white police officer in Minneapolis, Minnesota, killing a Black man by kneeling on his neck for nearly nine minutes. George Floyd’s death sparked protests that would spread through the country and the world over the course of two weeks. It’s too soon to know how these two events might affect the spread of coronavirus. Nonetheless, the hand-wringing about who to blame when the disease surge arrives—the states that had reopened too early or the protesters—has become a kind of Rorschach test of political preference.
But that dichotomy misses the point.
There was never a comprehensive plan to stop the novel coronavirus from infecting millions of people, much less preventing more than 100,000 deaths in the United States. In the early days of the pandemic, Donald Trump insisted that it would just go away. His party and favorite television network blamed it on a Democratic plot to sabotage Trump’s reelection chances. Larry Kudlow, who is the Director of the United States National Economic Council and not an infectious disease expert, insisted the contagion was contained. And when in doubt, China and the World Health Organization were the perfect scapegoats. Meanwhile, state and local governments scrambled to close schools and businesses, and ordered everyone to stay home in an effort to limit the damage.
The federal government failed spectacularly to roll out a competent strategy to test and isolate the sick, and the country first slowly then suddenly shut down. As the unemployment numbers climbed, the government gave a portion of the population a $1,200 check for their troubles. Then, the nation and the world watched in horror as US hospitals were inundated with people gasping for air, our morgues overflowed with bodies, our food distribution lines circled around the block, and millions of people applied for unemployment as the jobless rate soared. It remains a spectacular display of government incompetence and an indictment of the entire American system.
But then there is the question about the uptick in cases, just when we thought we were “flattening the curve” and states were reopening. This week, according to the Washington Post, several states have seen an increase in coronavirus hospitalizations in the last two weeks, the typical incubation period for COVID-19 and the period of time that has elapsed since Memorial Day. Texas, which was one of the first states to ease restrictions, has seen a 36 percent increase in new cases since the holiday. In Arizona, hospitalizations have increased by 49 percent. And in Arkansas, hospitalizations are up by 88 percent during that same time period. Several states are warning that their hospitals could soon be at capacity. Did this result in a renewed government effort to address the crisis? Hardly. Just more of the same, tired blame game.
Not that this reflex is unique to the pandemic or to police shootings. It’s a tried and true American reaction. When faced with systemic failures, we look at individuals not the system. For Black people who live in poverty, it’s not the decades of racist policies that have left them with a decimated tax base and crumbling infrastructure, it’s their fault for not pulling themselves up by their bootstraps. Earth is warming at an alarming rate, bringing with it untold disaster. But instead of blaming decades of corporate pollution for profit, and the complicity of certain elected officials to make sure there are no consequences, we shame people who drink out of plastic straws and neglect to bring their own woven shopping bag to the store. When the coronavirus appeared, the vast majority of people, those whose livelihood did not depend on placing themselves in harm’s way, mostly stayed home, wore masks when they went out, and sanitized their hands regularly. And still, even though that individual action may have slowed the spread, without any aggressive government intervention, the renewed surge of the virus could be even more deadly than the first round.
The government’s lackluster response to the pandemic is rooted in a president who is actively hostile to science, the systematic defunding and dismantling of government bodies like the pandemic response team in the National Security Council, and Trump administration interference with and undermining of the work of the Centers for Disease Control. The once world-class agency has largely remained silent or been muffled. As a result, we’ve all been left to decide on our own which activities are safest and how to minimize risk while we navigate the world while COVID-19 still spreads. And because we’re following our own rules, with few accepted government guidelines, it’s only natural to see photos of people doing something you personally don’t think is safe and to blame them for the current state of affairs. If only they were quarantining like me, we wouldn’t be in this mess.
Most public health experts agree that washing your hands, wearing a mask in public, and mostly staying at home is the best way to remain safe from COVID-19. But if you think everyone should stay home until there’s a comprehensive testing, tracing, and isolating strategy in place, you’ll be waiting for a long time. The Trump administration has not indicated that they’ll beef up the coronavirus response. In fact, it appears that they’re ready to move on and wage yet another culture war while Americans die by the thousands every week. As my colleague David Corn reported on Thursday:
[Trump] referenced the coronavirus crisis—”this horrible plague”—in his usual fashion: he defended his administration’s record on testing, and he blamed China for the pandemic. But he said nothing about the need to stay vigilant regarding masks, social distancing, and other countermeasures. (Trump even toured the plant without wearing a mask, and the swabs he watched being made in a sterile environment were later thrown out.) He said nothing about coronavirus remaining a serious threat to the United States.
If we weren’t in this unique moment, I might be inclined to believe that the predictable cycle of government incompetence and blaming individuals will continue indefinitely, certainly as long as Trump remains president and the Republicans remain in power. The government will fail to respond, hundreds of thousands of people will die, and we’ll accept it as just another facet of American life.
But for the first time in generations, a counter-narrative is beginning. There’s an uprising. More people are starting to realize that maybe there is something systemically wrong. A majority of Americans think the death of George Floyd represents a broader problem of policing. They’re realizing that we have the money to arm police officers with military equipment, but across the country people are forced to wait hours to cast a ballot. They see that the federal government can give corporations billions of dollars, but only offered a single payment of $1,200 to working people during the economic crisis, plus a temporary boost in unemployment benefits. It’s time to make the final connection and see that the same premise that there is something pervasively wrong with our system of policing also holds true for the pandemic.
Yes, there’s a crisis. But remember, fundamentally, we only have the government to blame.
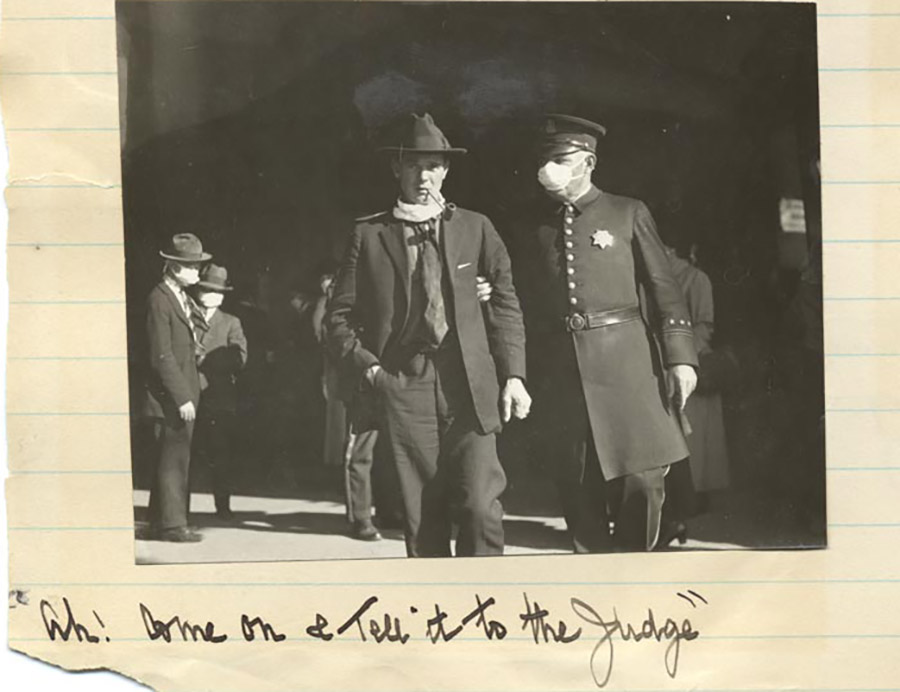
“Come on & tell it to the judge”: A man is arrested for not wearing a mask in San Francisco, 1918. California State Library
Take a walk in any park in the United States right now, and you may be tempted to believe that the coronavirus pandemic is all but over. Every state has loosened its lockdown restrictions, and the warmer weather has Americans eschewing sweaty masks to take in the summery air. Plus, hundreds of thousands of people across the country have congregated in the streets—with and without masks—to protest racial injustice, defying bans on large gatherings, albeit for a righteous cause. More Americans are going to work in person and the percentage of Americans who wear masks in public, which rose steadily in April, has leveled out at around 70 percent, according to data from YouGov. Still, many states are seeing COVID-19 case counts rise, and public health experts don’t expect the pandemic to resolve anytime soon.
If history is any indicator, attempts to reinstitute social distancing measures to flatten a potential second wave of the virus could face more opposition than the initial lockdowns. The widespread business closures and mask ordinances implemented during the 1918 influenza pandemic weren’t especially popular. Yet a second round of restrictions put in place to stem a second wave of the flu was so hated that dissenters in San Francisco formed a 2,000-person Anti-Mask League and some mayors openly violated public health orders. Similarly, it’s not hard to imagine the return of ferocious anti-lockdown protests if authorities enforce new lockdowns when COVID-19 counts start to tick back up.
To understand the echoes of the flu pandemic in our current moment, I contacted historian J. Alex Navarro. Navarro was one of the researchers who, as part of a Bush-era initiative to prepare for for a possible pandemic, helped the Centers for Disease Control and Prevention by studying newspaper archives from 43 American cities to determine whether social distancing measures during the 1918 outbreak reduced mortality. (They did.) Navarro, along with Dr. Howard Markel, is coeditor-in-chief of the online Influenza Encyclopedia, which hosts a fascinating page about the anti-mask sentiment that abounded in 1918 San Francisco.
I spoke with Navarro about a historical constant: humans’ tendency to buck authority, even if it means putting their health at risk.
Abigail Weinberg: What major political differences should we be aware of when comparing 1918 to today?
J. Alex Navarro: In 1918, there’s this overriding sense of hyper-patriotism that is not only being driven by the war effort, but is also being purposefully stoked by [President] Woodrow Wilson. It was not a very popular war, so Wilson created the Committee on Public Information, basically a propaganda effort. Patriotism is being ginned up as much as possible, and that probably had a large effect on the initial reaction to the epidemic from the public.
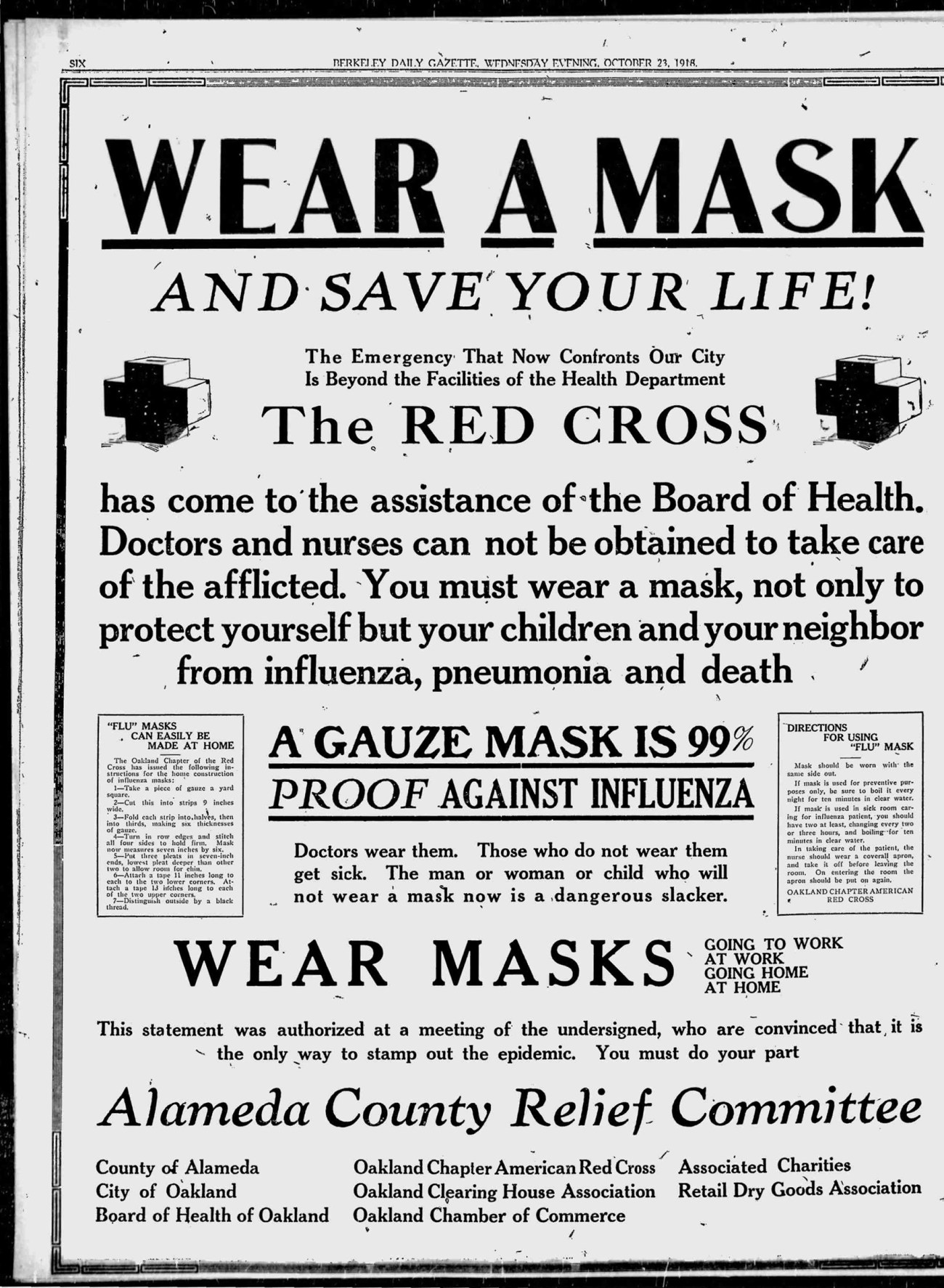
You can see this in the newspaper coverage. For example, in places where mask ordinances were passed, like San Francisco, the Red Cross prints out this PSA in the newspapers and basically says, “Save a life. Wear a mask. Do your part.” It actually used the term “slacker,” which had been used for people who weren’t doing their part to support the war effort.
A Red Cross advertisement that appeared in the Berkeley Daily Gazette on Oct. 23, 1918
In what ways did people resist or defy public health measures?
There were some notable acts of pushback, from actual legal challenges to outright defiance. For example, about three weeks into Atlanta’s epidemic, a group of businessmen come to the mayor, Asa Candler, and they say, “We need to reopen.” He’s a pro-business leader, and he decides unilaterally, over the objection of his board of health, to reopen Atlanta—and Atlanta’s epidemic was not over. In fact, we don’t really know the course of Atlanta’s epidemic, because the city stopped reporting cases in the same way. [Sound familiar?]
In San Francisco there were two mask orders, but it’s the second one in January of 1919 that leads to this Anti-Mask League. Even during the first mask ordinance in the fall, there are hundreds of people who are arrested for not wearing their masks. It’s hard to know how many of those people were being defiant because they just didn’t think that they needed to wear one, or the government had no right to tell them to wear one. Some of them probably simply forgot or thought they could get away without wearing a mask because they were uncomfortable, but they got caught and were arrested.
But then it leads to that second mask order when there’s a resurgence in cases, and that one was definitely despised. People did not like wearing the masks, and there was opposition from prominent physicians. There was a member of the California Board of Supervisors who was part of the Anti-Mask League. There were 2,000 people who met in an auditorium to hear speeches to protest the wearing of masks.
Perhaps the most notable example of defiance came from the mayor of Newark, Charles P. Gillen, who implemented the state Department of Health’s closure orders, which closed many places of public amusement including saloons, but at the last minute changed the saloon order and allowed them to sell liquor by prescription out of their side doors. Saloons took that to mean they could more or less remain open, which they did. They flagrantly flouted the ordinance. When the state department of health pushed back, Gillen didn’t back down, and he said that he was in charge of the Board of Public Health in Newark and that the state had no jurisdiction. He at one point decides that the epidemic’s over. It wasn’t quite over, he lifts the orders, and he said everyone can go back to life as normal.
How did Gillen’s constituents feel about his defiance?
Church leaders were not happy that churches were required to close, but saloons were basically allowed to be open. They complained to Gillen, and Gillen said, “If you want to reopen, I’m gonna look the other way at churches.” The Newark Evening News was aghast that he would do this, and they ran scathing editorials about the mayor. He in fact ordered them out of his office. He said, “None of your reporters are welcome until you stop printing lies.” He had no authority to do it, but he threatened to close the newspaper down under public health rules for being a public health nuisance for questioning his authority. It’s kind of reminiscent of what’s going on today.
People who refused to wear masks in 1918 claimed that they were ineffective or that mask ordinances were unconstitutional—many of the same justifications we hear today. How did the Anti-Mask League differ from the vocal minority of anti-mask protesters that we see on the news today?
In terms of why there was such widespread organized opposition in San Francisco in particular, I think that has to do with timing. Denver, Seattle, Oakland, and San Francisco all used masks, and they were all hated in each of these cities. There was definitely opposition to wearing them. The difference, I think, in San Francisco, is San Francisco implemented a second mandatory mask order that came after the end of World War I, so that sense of patriotism and doing your duty is starting to dwindle. In other communities those mask ordinances ended right around or shortly after Armistice Day, so that patriotism is still hanging around a little bit, and then as it starts to dwindle, people want to get back to life as normal. That’s when San Francisco rolls out this second mask order.
Did the virus disproportionately affect minorities and lower-income communities, as we’re seeing today?
We don’t really know, and that’s because the data just doesn’t really exist. We don’t even know the number of aggregate cases.
Chicago had a very long, very detailed public health report on the pandemic. They do include some racial data, but it’s really interesting the way they include it. They calculated the percent change increase in the number of deaths for whites versus African Americans due to the epidemic, and what they found is that that percent change was much higher for whites. They concluded therefore that Black residents may have had some sort of immunity to influenza. It’s not at all the case. It’s just that the way that they reported and were looking at the data, if you have a group of people who are already dying of other underlying medical conditions at a higher level than their white counterparts, then the epidemic comes along and kills people at roughly the same level, probably more heavily impacting African Americans, the difference in that decrease is going to be much greater for the group that had fewer underlying health conditions and better access to health care initially. So the percent change seemed greater for whites than Blacks, but the reality was that was because African Americans were already dying from other endemic diseases and malnourishment and diseases of that sort at higher levels.
“Get a mask or go to jail.” California State Library
The coronavirus in the United States has stoked xenophobia and racism against Asian-Americans, particularly people of Chinese descent. Given that epidemics have historically lent themselves to scapegoating, did the 1918 flu exacerbate racism in the United States?
It probably did not exacerbate racism. This is probably the first pandemic, in fact, where we don’t see widespread scapegoating. There is one example that comes to mind. When Denver released its closure orders on Armistice Day, there was a great rush for everyone to congregate downtown and celebrate. They had another spike in cases that was actually worse than the first spike. A public health official for the city complained that that second spike in cases was caused by Italian and Hungarian immigrants, because they were congregating to care for sick relatives and friends. That is probably true. They probably were. Culturally, people from various communities probably were likely to take care of each other, especially if you live in a community like Denver which had a history of anti-Italian prejudice. But to blame them for causing the continuation of the epidemic was of course completely inaccurate. But that’s the only case that we saw of that, and I think it’s pretty striking.
Why do you think cases of scapegoating were so rare?
I think because it hit so hard and across all segments of the population—all ethnicities, all racial groups—with equal ferocity, that you couldn’t easily pinpoint it to a particular group of people and then scapegoat that group of people. It seemed to pop up out of nowhere.
Public health crises tend to spawn misinformation. I’m sure you remember the president suggesting that people ingest disinfectants to cure the coronavirus. Were there any dangerous folk remedies in 1918 that people had to look out for?
There were lots, and they range from dangerous to silly. One of the typical ones was “clean heart, warm feet, clean bowels.” Some people advocated cutting an onion in half and rubbing that on your chest and that would protect you. There may have been something to that: If you smell like raw onion, people are probably gonna stay away from you. There were some who recommended taking a bath of creosote—which is a pretty dangerous, toxic chemical—and taking copious amounts of brown sugar.
What lessons can we take away from studying the 1918 pandemic?
These closure orders are very onerous for society as a whole, particularly business owners, but they’re meant to just initially get a handle on an explosive pandemic. They’re not meant to be in place forever. As we come out of this and as we see states starting to reopen, if we don’t have an effective mitigation strategy in place that people are actually going to use and buy into, that’s a huge problem.
In 1918, when cities removed these social distancing orders and closure orders, in cities that faced another spike in cases when the epidemic wasn’t quite done yet, it was almost impossible to reimplement closure orders a second time, because the business community in particular and residents overall pushed back so much. Today, if we’re not gonna do things like socially distance whenever possible, if we’re not going to wear masks while in public and get widespread compliance, I don’t see how we mitigate the pandemic as it rolls on.
This epidemic will be around with us for a lot longer than influenza, because the threshold for herd immunity is at least twice as high for COVID. Human nature being fairly static despite changes in historical context, I fear that whatever the level of opposition is now—it seems small but rather vocal—that that’s gonna turn into a combination of outright defiance and noncompliance.
Immigration detainees sit in a yard at the Winn Correctional Center, a for-profit prison in Louisiana run by LaSalle Corrections, in September.Gerald Herbert/AP
A fourth guard at a US immigration detention facility has died as a result of COVID-19, as the virus continues to spread through the close quarters where asylum seekers and other immigrants are being held indefinitely.
On May 1, Lieutenant Lewis Dempsey was sent home from a Louisiana immigration detention center with a fever. On Wednesday morning, he passed away from complications from COVID-19.
Dempsey is the third employee of the private prison company LaSalle Corrections known to have died after contracting the new coronavirus. All three are assumed to have been infected at Immigration and Customs Enforcement detention centers in rural Louisiana where 180 people in detention have now tested positive. The first two both worked at the Richwood Correctional Center. Dempsey worked at the Winn Correctional Center. A fourth guard employed by another private company, CoreCivic, at an ICE detention center in New Jersey died in April.
Dempsey’s death is a reminder that it is not just immigrants whose lives are put at risk by ICE’s decision to keep people in crowded detention centers. Detention center employees, their families, and their communities are also threatened by the outbreaks that experts warned for months were inevitable. As of Wednesday, 115 people detained at Winn have tested positive, 45 of whom are still being monitored for COVID symptoms.
Twopeople died in ICE custody last month of complications from the new coronavirus. A third man died after being released from a detention center with a massive outbreak without being tested.
LaSalle spokesperson Scott Sutterfield, who previously served as ICE’s top official for Louisiana and four other Southern states, said about Dempsey, “We were saddened to learn today of the passing of our friend and colleague. Our thoughts and deepest sympathies go out to his family, friends and coworkers.” ICE did not immediately respond to a request for comment. The agency does not report when employees of the private prison companies it contracts with test positive or die.
Former Mother Jones reporter Shane Bauer worked as a guard at Winn while it was a Louisiana prison operated by CoreCivic. His award-winning investigation exposed an institution plagued by rampant violence and medical neglect. Last year, I reported that ICE had started sending immigrants and asylum seekers to the facility:
The prison, which is more than four hours from both Houston and New Orleans, is in the “middle of absolute nowhere,” [Marshall Goff, a Mississippi immigration attorney,] says. When he visited for the first time on Saturday, it was clear to him that it was designed to be a prison, not a jail that holds people serving short sentences. It was striking to Goff that immigrants, who are held in a separate area of the prison, “are being housed in the same place as people who commit felonies and who’ve been sentenced for decades.”
The GoFundMe page started by Dempsey’s sister Dochia Doughty states that he was initially unable to get non-emergency medical attention in Winnfield, the town where the detention center is located. He was later rushed to the local hospital, where he nearly died before being airlifted to Shreveport. Dempsey would go on to “code,” a term used when people go into cardiopulmonary arrest, many times there.
His family still hoped that he would survive when they started a GoFundMe page to raise money for his recovery on Tuesday. Doughty wrote about her brother:
Our family is just an ordinary, working-class American family, but we do have extraordinary work ethic. Lewis was undeservedly struck by an extraordinarily deadly virus. Yet he survived. This is a long and on-going story, but what happened to Lewis could happen to any of us. While he may be an ordinary statistic to some, he is an extraordinary brother to us. He epitomizes a loving, kind-natured man with a childlike innocence. I always say he’s a lover, not a fighter. We place no blame or fault on anyone.
On Wednesday morning, Doughty updated the fundraising page to say that her brother had passed away. “My sister and I were allowed in to love on him beforehand,” she wrote. “He was alert and listening to us. His heart just stopped. He left this world knowing he was loved by so many family and friends.”
Two children cross the Rio Grande into the United States to turn themselves over to authorities and ask for asylum. June 2019.AP Photo/Christian Torres
The Trump administration is facing the first legal challenge of its policy of turning away thousands of asylum seekers at the southern border—including unaccompanied children—during the coronavirus pandemic.
The ACLU and others filed a lawsuit in federal court Wednesday on behalf of a 16-year-old Honduran boy who was set to be deported after coming to the United States last week to flee persecution at home. A federal judge temporarily blocked the deportation, however, following the filing of the suit.
The government’s move to deport the boy was in line with an emergency order issued by the Centers for Disease Control and Prevention that suspended immigration into the country as a way to prevent the spread of the coronavirus. But the ACLU is arguing that the boy’s expulsion from the country would violate anti-trafficking laws and special protections afforded children seeking asylum.
The CDC order was issued in March—and extended indefinitely—ostensibly as a measure to protect the health and safety of Americans. But it has effectively shut down the immigration and asylum systems at the southern border. In recent months, thousands of asylum seekers have been turned away there, and the Office of Refugee Resettlement, which would normally house minors while they are being placed with family members or sponsors, has seen a dramatic decline in new immigrants entering its care—just 58 for the month of April, according to BuzzFeed News.
Immigrant advocates say that the Trump administration is merely using the pandemic as cover to push through its draconian immigration policies. As Andrea Flores, deputy director of immigration policy for the ACLU, told my colleague Fernanda Echavarri last month: “The president is hellbent on exploiting a public health crisis to achieve his long-held goal of ending asylum at the border. He’s also doubling down on fear-mongering against immigrants, so many of whom are essential workers during this crisis. Do not be fooled: Trump’s goal is not to protect our health, it’s to sow division and advance his political agenda.”
A window at the Cook County jail complex.Scott Olson/Getty
From the earliest days of the pandemic, criminal justice experts and advocates warned that jails could rapidly become major sources of infection as staff and inmates enter into crowded and unhygienic conditions, then return to their communities outside. Now, research has revealed just how significant a role the Cook County Jail—one of the country’s largest—has played in spreading the coronavirus: Nearly 1 in 6 COVID-19 cases identified in all of Illinois by mid-April was associated with people cycling through the jail, according to a new analysis.
The paper, published Thursday in the journal Health Affairs, used booking, release, and infection data from the Cook County Jail and coronavirus case counts from the Illinois Department of Public Health to analyze the relationship between “jail cycling”—high rates of people being arrested and released—and coronavirus infection rates across different neighborhoods. COVID-19 case rates, the authors concluded, were “significantly higher” in zip codes where many people were cycling in and out of jail. Jail cycling was even more strongly associated with a zip code’s COVID-19 case rate than race, poverty, public transit utilization, or population density.
“Although we cannot infer causality, it is possible that, as arrested individuals are exposed to high-risk spaces for infection in jails and then later released to their communities, the criminal justice system is turning them into potential disease vectors for their families, neighbors, and, ultimately, the general public,” the authors wrote. Given just how disproportionately Black neighborhoods are policed, they added, the powerful role of jails in spreading infection “may bear partial responsibility” for the wide racial disparities seen in coronavirus case rates. Black residents comprise 30 percent of the population in Chicago, but accounted for 52 percent of the city’s COVID-19 cases as of early April, according to the Associated Press. (As of June 4, the city was reporting that 30 percent of its coronavirus cases were among Black residents; 48 percent were among Latinx residents.)
Every person who cycled through the jail translated to 2.149 new cases of COVID-19 in the broader community, explains co-author Eric Reinhart, a PhD student at Harvard University and medical student at the University of Chicago. This means that the 2,129 people released from Cook County Jail in March were associated with an additional 1,938 community infections in Chicago, and 4,575 community infections in all of Illinois by April 19. Since then, the numbers have likely only grown. “There is a cascade effect,” Reinhart says in an email. “Each of these infections subsequently multiplies into more cases with more people.”
Reinhart argues that the study’s results reveal consequences of a “a much broader structural problem of hyper-aggressive arrest practices and mass incarceration across the country.” But the particular role of the Cook County Jail in spreading infection should come as no surprise. As my colleague Samantha Michaels reported in April, a federal lawsuit seeking the release of inmates at higher risk for COVID-19 described the impossibility of following public health guidelines inside:
The class-action lawsuit includes Anthony Mays, a 38-year-old with diabetes who was referred for an evaluation for a heart condition when COVID-19 hit the jail. He’s housed in an open-dorm setting where dozens of beds are spaced about two feet apart, and multiple detainees on the tier have been removed after testing positive. Kenneth Foster, another plaintiff, also lives in a dorm setting and has stomach cancer, lung sarcoidosis, high blood pressure, asthma, and bronchitis. Other inmates named in the suit have Hodgkin lymphoma and blood clots; one man’s throat was reconstructed after he was shot.
“Inside accounts from Jailstaff, detainees, and…medical personnel paint a picture of an unfolding disaster,” states the lawsuit, filed by civil rights attorneys who argue the county has violated people’s constitutional rights by failing to protect them from disease at the jail. The roughly 4,700 detained men and women at the Cook County Jail share phones, toilets, sinks, and showers, often with limited access to soap and hot water. Surfaces are infrequently washed, according to the suit, and people are quarantined in group settings, not individual cells, increasing the chance of infection. “It’s a lot of people, who were in a very intimate physical space with someone who is positive,” says Stephen Weil, one of the attorneys.
For the past several months, the Cook County Jail had been reducing its population in response to the pandemic. But over the past week, the trend has reversed, as police arrest large numbers of people during protests against police brutality and systemic racism. In May, about 4,000 people were incarcerated, according to local news station WTTW. By Thursday, that number surpassed 4,500.
Update, Friday June 5, 8:00 p.m.: In a statement, the Cook County Sheriff’s Office argued that the Health Affairs study was based on outdated information. “As a result of our interventions, cases at the jail have dropped precipitously over the past month,” said assistant director of public relations Kathleen Carmody. At present, the jail has identified 36 detainees and 42 staff members who are positive for COVID-19, according to Carmody; 511 additional detainees who have recovered from COVID-19 were still in custody as of Thursday.
Over the past few months, there has been a pretty heated debate raging in both scientific and political circles over the antimalarial drug hydroxychloroquine. The broad outlines are likely familiar at this point: President Trump has touted its effectiveness to treat COVID-19, even claiming to be taking it himself as a preventative measure, without scientific evidence to back him up and even though the FDA has warned against its use outside of hospital settings.
Now there’s a new development: On Thursday, researchers retracted a major study that suggested a link between hydroxychloroquine and a substantially increased risk of death. Another leading journal has issued a statement that questions the integrity of related research.
The now-retracted study, which published last month in the Lancet, a respected research journal, included analysis of 96,032 patients’ records and was at the time the largest study to investigate the drug’s potential in fighting COVID-19. According to the study, patients who received a cocktail of hydroxychloroquine and an antibiotic saw a 45 percent increased risk of death. The news was a big deal. Several media organizations, including Mother Jones, picked up the study. The World Health Organization, which had been investigating hydroxychloroquine’s potential as a coronavirus treatment, paused recruitment for its trial. And Italy, France, and Belgium banned the drug from being used to treat COVID-19.
Still, questions about the study started popping up shortly after it published; more than 180 researchers issued a letter raising potential problems with the data behind it, and on May 29, the Lancetcorrected some of the data. Now, just shortly after the Lancet and the New England Journal of Medicine published “expressions of concern” about the research, the authors have officially retracted the paper.
“Today, three of the authors of the paper, ‘Hydroxychloroquine or chloroquine with or without a macrolide for treatment of COVID-19: a multinational registry analysis’, have retracted their study,” the Lancet announced in a statement. “They were unable to complete an independent audit of the data underpinning their analysis. As a result, they have concluded that they ‘can no longer vouch for the veracity of the primary data sources.'”
NEJM, which published a study on May 1 drawing from the same data source, wrote in an expression of concern, “Recently, substantive concerns have been raised about the quality of the information in that database. We have asked the authors to provide evidence that the data are reliable.”
Without access to the data, it’s unclear what exactly, if anything, went wrong, though I recommend you read this excellent investigation by the Guardian into the company that provided the dataset. But what we do know now is that the controversy is concerning—if not unsurprising, given how fast the science is moving around COVID-19 and how desperate people are for information on the disease that’s claimed more than 100,000 American lives.
As I’ve written before, experts say the pandemic has put a strain on an already flawed scientific review process. The coronavirus has brought on a deluge of manuscripts for journals to review. Multiple journals, including NEJM, told me in April that their peer-review process has been expedited. But even in normal times, peer-reviewed journals often don’t review raw data as part of the vetting process in the first place. “I would argue maybe they should more often because that might prevent cases like this,” Ivan Oransky, a founder of Retraction Watch, a blog that tracks academic retractions, told me earlier this week after the Lancet study had been flagged for concern, but before it was retracted; Oransky also serves as the vice president of editorial at medical news and reference site Medscape and teaches medical journalism at New York University. “Journals hardly ever look at the underlying data.” Other times bias and error simply slip by peer-reviewers.
When Mother Jones asked the Lancet via email on Thursday how this paper made it past peer-review, the journal did not answer directly. It instead underscored that the paper was, in fact, peer-reviewed. “All research articles published in The Lancet journals undergo independent, external peer review, including statistical review,” it wrote. (NEJM simply told Mother Jones that the expression of concern “must speak for itself for now.”)
The Lancet study in question is one of a handful of COVID-related papers that have been retracted already, though this might be the most high-profile. So far, Retraction Watch has documented 14 retractions (including today’s) and two temporary retractions for recent coronavirus-related research, as well as two expressions of concern about COVID-19 papers (including NEJM‘s notice this week).
Generally speaking, expressions of concern are not common in the science world, but they’re not unheard of either. “An expression of concern is used when editors have a reasonable sense that there might be something wrong but they’re not sure yet. So it’s not a retraction, but it’s grander than a correction,” says Oransky. Retractions are more serious. On average, according to Oransky, the amount of time between when a paper is published and withdrawn is about three years. Again, the pandemic has put this entire timeline into super-speed.
Both papers using this now-disputed data were authored by a team of researchers led by Dr. Mandeep Mehra, a professor of medicine and a cardiovascular specialist at Harvard Medical School. A co-author is Sapan Desai, who leads Surgisphere, the data firm which supplied the COVID dataset for the studies. The Guardian investigation raises a slew of concerns about the validity of the data, including significant data discrepancies and conversations with hospitals that said they did not participate. It also reports that Desai “has been named in three medical malpractice suits, unrelated to the Surgisphere database” and that several of the company’s employees have “little or no data or scientific background.” (Again, it’s worth reading the Guardian‘s investigation in full.) Despite pleas from the scientific community, the authors of the initial study have yet to supply the raw data from the studies, citing confidentiality concerns.
Complicating matters on hydroxychloroquine even further, the first major controlled clinical trial of the drug was published on Wednesday in the New England Journal ofMedicine and found that it does not help prevent infection. As the New York Timesreports:
The malaria drug hydroxychloroquine did not prevent Covid-19 in a rigorous study of 821 people who had been exposed to patients infected with the virus, researchers from the University of Minnesota and Canada are reporting on Wednesday…. Conducted in the United States and Canada, this trial was also the first to test whether the drug could prevent illness in people who have been exposed to the coronavirus.
…
“The take-home message for the general public is that if you’re exposed to someone with Covid-19, hydroxychloroquine is not an effective post-exposure preventive therapy,” the lead author of the study, Dr. David R. Boulware, from the University of Minnesota, said in an interview.
Though both dispute the effectiveness of hydroxychloroquine, this new NEJM study and the now-retracted Lancet study have highly different methodologies. The Lancet paper was observational: The researchers had no control over who received or did not receive treatment. A controlled clinical trial, on the other hand, which happened in the new NEJM study, is a much more rigorous experiment (though it’s still not foolproof).
If there’s one definitive takeaway this week it’s that the research is moving quickly. And a lot of it is incomplete. At a time when we need good science the most, experts tell me bad science is slipping through the cracks at an alarming rate. “What [the pandemic] has done is just made everyone rush to publication and rush to judgment, frankly,” Oransky told me in April. “You’re seeing papers published in the world’s leading medical journals that probably shouldn’t have even been accepted in the world’s worst medical journals.”
Let’s pretend it’s the year 2021. After rigorous clinical trials, the FDA confers a license of approval, and we finally have a safe and effective vaccine against the novel coronavirus. One problem is solved but a host of others follow. How can everyone be convinced that it’s safe and effective? How can enough be produced for the 7-and-a-half billion people on the planet who will need it? Even if there are sufficient supplies and a buy-in from those opposed to vaccinations, given how contagious the coronavirus is, how can there be mass inoculations without forcing people to congregate in ways that further spread the disease?
These are the questions with which public health officials, epidemiologists, and logistics companies are grappling. “It could be a great vaccine, but if you can’t get it to people it doesn’t count,” said Dr. Jon Abramson, a professor in the pediatrics department at the Wake Forest School of Medicine, a member of vaccine advisory groups at the World Health Organization (WHO), and the Global Alliance for Vaccines and Immunizations (Gavi). He currently serves on two different coronavirus vaccine working groups. According to Abramson, more than 120 labs and companies worldwide are working toward creating a safe, effective vaccine.
In the most high-speed vaccine development program in human history, the Massachusetts-based biotech company Moderna jockeyed into first place in the last couple of weeks. Last Friday, the company announced it was starting Phase II clinical trials. This was after eight participants in a Phase I clinical trial for its mRNA vaccine showed antibodies comparable to patients who have recovered from COVID-19. Moderna’s stock prices soared, top executivessold off $30 million of stock, and its early successes were significant enough that even the administration’s most trusted voice during the pandemic, Dr. Anthony Fauci, head of the National Institute of Allergy and Infectious Diseases, expressed cautious optimism that we could have a vaccine sooner than expected. “It is conceivable, if we don’t run into things that are unanticipated setbacks, that we could have a vaccine that we could be beginning to deploy at the end of this calendar year, December 2020, or into January 2021,” he said in a May 22 interview on NPR’s Morning Edition.
Given the four phases involved in the development of any vaccine, there are a number of different points where the “unanticipated setbacks” that Fauci had warned about could derail the process. It might happen during research and development, or during the three phases of clinical trials required before any drug is made available to the public. Manufacturing large amounts will be difficult because vaccine materials are expensive and sensitive. Distributing the serum all over United States, not to mention all over the world, is a massive undertaking. Vaccines are biologic substances, vulnerable to heat, light, shock, and humidity. They need to be stored in special, industrial-sized pharmaceutical refrigerators at specific temperatures, usually between 2 and 8 degrees Celsius, for their entire journey from factory to hospital. And that’s all before a single dose is administered, and those logistics may be the most daunting of all.
The two most advanced vaccines in the running—Moderna’s and theOxford vaccine—are entering Phase II of the clinical trials stage, in which the vaccine goes from being tested on a small group of subjects to being tested on thousands of subjects. After Phase II, there will be one more phase of trials, involving thousands of subjects to demonstrate its safety and efficacy. But clinical trials won’t be the most difficult part. Fauci said the speed with which vaccines are coming to market can strain the production process, disrupting the economic models for manufacturing and funding. To develop a vaccine as quickly as possible, the governments will be investing in and even paying companies to make doses of vaccines that might never work. “The risk is not to the patients,” said Fauci. “The risk is to the investment.” He means that massive sunk costs in the past have deterred pharmaceutical companies from manufacturing vaccines.
After a vaccine passes through the stringent clinical trials and the US Food and Drug Administration’s licensing process, it is up to the Advisory Committee on Immunization Practices (ACIP) at the Centers for Disease Control and Prevention to give federal recommendations about how the vaccine should be administered. Dr. José Romero, the current chair of ACIP, is concerned about the challenges of producing enough vaccine for the entire US population, and the disparities that might result in its distribution. “A single vaccine manufacturer, up until this point, would not be able to produce enough vaccine for the entire population,” he said. “Will there be enough syringes, will there be enough vials to administer vaccine to millions of people in our country?”
Moreover, he notes, “It’s well known that the ravages of this infection have struck hard in minority groups. It’s shone a light on healthcare disparities in this country.”
Lacking any direction that could come from a coherent national policy, states have largely had to improvise their response throughout the pandemic. In much the same way that states have taken varying approaches to following the CDC’s recommendations on re-opening the economy, state health departments could adopt a variety of approaches in contracting with vaccine manufacturers and implementing a campaign. ACIP can only give recommendations. They have no authority to enforce them.
Producing mass quantities of whatever vaccine crosses the finish line first will also require producing mass quantities of needles, vials, disposal units, and protective equipment for health workers performing the inoculations. Abramson, who used to chair ACIP and is currently on multiple vaccine working groups, noted, “There will be supply issues, but they are already thinking about that. We learned our lesson the hard way with PPE.”
On April 2, Bill Gates, who has invested $300 million into fighting the coronavirus, went on The Daily Show. After making a fortune as the creator of Microsoft, Gates and his wife, Melinda, have invested billions of dollars into public health efforts through the Gates Foundation. The Foundation has led a global effort that has helped immunize more than 700 million kids and saved an estimated 6 million lives.He explained that the US government’s response to the coronavirus should be analogous to how the government prepares for war. “Every state is being forced to figure things out on their own. It’s very ad hoc,” said Gates. “It’s not like when a war comes, and we’ve done 20 simulations of various types of threats, and we’ve made sure that the training, communications, logistics, all those pieces fall into place very rapidly.”
He also shared his plan to prepare simulations for various types of vaccine manufacturing. With its previous successfighting diseases through vaccine alliances, his foundation is starting to build factories for seven of the potential vaccines in development. “Even though we’ll end up picking at most two of them, we’re going to fund factories for all seven,” he said. “It’ll be a few billion dollars we’ll waste on manufacturing for the constructs that don’t get picked.” Gates’ high visibility in the development of a coronavirus vaccine has made him the target of right-wing conspiracy theorists, despite the fact that his funding will likely be critical to getting massive amounts of the vaccine manufactured quickly—or maybe because of it.
Manufacturing sufficient amounts of the vaccine will do nothing until it gets to everyone across geographical and economic boundaries, in all ages and stages of life. Andrew Schadegg is president of Unitrans, a subsidiary of AIT Worldwide Logistics, a company that distributes products globally by air, land, and sea. Schadegg’s company is responsible for transporting vaccines and biologic drugs from factories to distribution centers, and then from distribution centers to administration sites, like pharmacies, hospitals, and doctors’ offices. “I’m not familiar with ever having a situation where that amount of product was needed to be manufactured and then shipped to all these different sites,” he said. “So that’s going to be a challenging one.”
Schadegg says that rolling out a coronavirus vaccine is logistically possible because the infrastructure is already in place. “You have distribution centers, you have temperature-controlled trucking. The technology is there to support this,” he said. “The global pharmaceutical companies have already been able to vaccinate large parts of the world in much more challenging environments.”
In normal times, about half of global air cargo is moved on passenger flights. But with most passenger flights canceled due to the pandemic, the entire global air freight system is under stress. Vaccine development is part of a global supply chain system. A turbulent trade environment makes it difficult to plan for vaccine deployment. “We’ve had a quasi-trade war with China for a long period of time and that’s been very disruptive to global supply chains,” said Schadegg. “Vaccines or pharmaceuticals are definitely involved in the global supply chain, so it’s key to not have a massive trade war break out.”
Matthew Watson, a senior analyst at Johns Hopkins University’s Center for Health Security and his colleagues have been paying particular attention to the vaccine’s distribution and administration. How will it be possible to administer a traditional injectable product to people who are not yet infected, who do not have immunity, and for whom waiting in long lines or congregating in doctors’ offices would be dangerous? With health care work forces already depleted, there might be a shortage of workers who can actually give the shot. That’s why Watson has been looking into alternative methods, like microneedle patches or tablets, that people might be able to receive in the mail and administer without the assistance of a health care professional. Plus, innovating how vaccines are administered could speed up the process during a future pandemic.
“It is notable that the two most successful eradication campaigns that we have on record are smallpox and polio,” Watson noted, “and they were administered not using a needle and syringe but using sort of an alternative route of administration.”
The poliovirus was a highly infectious disease that devastated populations around the world since the early 1910s, with especially bad outbreaks in cities like New York. It particularly afflicted children, killing and paralyzing tens ofthousands. Finally, the polio vaccine, discovered and developed by Jonas Salk, was licensed in 1955, and a mass program began to vaccinate children and teenagers. This was the era before the Federal Vaccination Assistance Act of 1962 and no nationwide immunization program yet existed. The NYC Department of Health relied on massive publicity campaigns to convince its population to voluntarily get the vaccine.
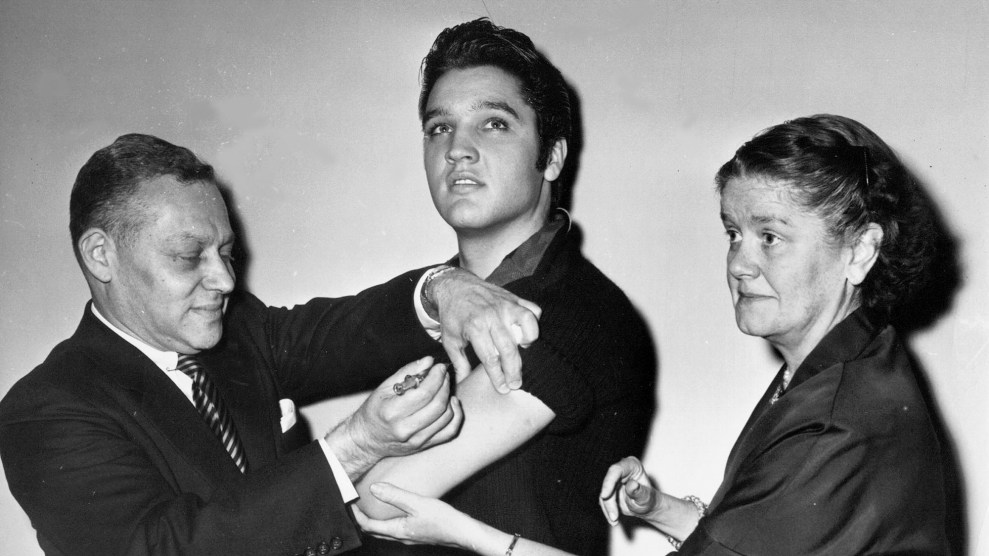
And that’s why, on October 28, 1956, Elvis Presley appeared on The Ed Sullivan Show, a staple of Sunday night television from 1948 to 1971. Elvis played his guitar. Hewarbled his upbeat bluesy music and made eyes at the live audience. He swiveled his hips so seductively that the cameras only shot him from the waist up during future appearances because it was a “family show.” After he stopped singing, he was joined onstage by New York City Health Commissioner Leona Baumgartner and Assistant Commissioner Dr. Harold Fuerst. Baumgartner cupped the King’s left elbow as Fuerst plunged a needle into the same arm. And, with that, Elvis Presley was injected with the polio vaccine.
Photos of Elvis getting inoculated ran in all the major newspapers. Commissioner Baumgartnersent Elvis a letter after the event, thanking him “for letting us publicize your polio shot and for appealing to teenagers to get vaccinated.” Children and teenagers lined up and were vaccinated, first from a shot and later from a droplet of vaccine on a sugar cube. Today, polio is almost entirely eradicated worldwide. But the time when a straight-forward public awareness campaign could work in America is over. The climate of suspicion around vaccines has grown so thick, the distrust of authority runs so deep, the power of social media to amplify conspiracy theories is so potent, that it will require more than a simple celebrity photo to inspire the necessary confidence for vaccinating millions.
When it is finally created, it is likely there won’t be enough vaccine available, so epidemiologists and public health professionals are concerned about massive inequities between the inoculated haves and have-nots. If certain populations don’t have access to the vaccine, the global population remains at risk. On April 24, theWHO organized a virtual meeting in which leaders from around the world agreed to cooperate on a coronavirus vaccine and distribute it around the world. The United States notably was absent. So was India, a major manufacturer of vaccines, especially for developing countries. Public health officials worry that this could replicate what happened during the 2009 H1N1 flu pandemic, when developing countries only got small quantities of the vaccine after wealthy countries got the amount they wanted.
The coronavirus vaccine might shift resources away from other vaccines and biologic drugs. Last year,twice as many people in the Democratic Republic of Congo died of measles than Ebola, which demonstrates that as sophisticated as global pharmaceutical supply chains have become, we are still operating in a world of finite resources. Measles has not received the same attention or investment as Ebola, so the resources have been uneven. These disparities are especially stark in countries where it’s nearly impossible to keep vast amounts of biologic drugs in temperature-controlled facilities.
Challenges notwithstanding, we are likely to see the fastest, most sophisticated rollout of a vaccine campaign in human history. “From a scientific point of view, it’s incredible to think that from November until now, we’ve moved from identifying this virus to now developing a vaccine,” Romero said. “This is unheard of. In my lifetime I’ve seen the acceleration in the development of drugs and vaccines due to molecular virology and molecular biology. This is the fruit of that. It’s just phenomenal.”
Yet, even as the science of vaccine development has advanced at “warp speed,” the social climate around vaccination seems to have moved backward.Anti-vaccine groups on Facebook have already exploded with conspiracy-laden coronavirus content, like theories that the coronavirus does not exist and claims that social distancing protocols are tactics of the “police state.” Once a fringe group, the anti-vaccination movement has amassed real power—enough to potentially derail the success of a new vaccine campaign. Dr. Myron Levine, associate dean for Global Health, Vaccinology, and Infectious Diseases at the University of Maryland, has seen the impact of the anti-vaccine movement on vaccinology, a discipline he helped establish. “We have a big problem of folks saying they have a right to determine whether their child should receive vaccine,” he said. “A highly infectious virus like measles can come back.”
On a morning walk through Brooklyn, as I wandered past the shuttered shops and restaurants in a city where more than 16,737 people have died from COVID-19, I was thinking about how a vaccine could not come quickly enough. In an effort to learn even more, I typed “vaccine” into the search bar in Apple Podcasts and clicked on the first podcast that popped up—something called “The Vaccine Conversation.” After about 10 minutes of chitchat between Melissa and Dr. Bob, and numerous references to “data” and “the World Health Organization,” I realized that that they were calmly making the case that the dangers of the coronavirus had been grossly exaggerated. In my earbuds, Melissa explained that the economic shutdown is an overreaction and wondered why the government wasn’t describing“things you can do to boost your immune system” like increasing vitamin D or “reducing sugar.”
“The Vaccine Conversation” has beendownloaded almost 400,000 times in over 90 countries, and it’s but one podcast within a vast media ecosystem of vaccine skepticism that is slowly shifting Americans’ attitudes. The antivaxx movement has already resulted inincreasing cases of measles where they were once thought to have been eradicated.Two-fifths of adult Americans now express anti-vaccination policy attitudes due to perceived links to autism, andanti-vaxxers have been a vocal presence at protests to reopen the economy in states like California and Colorado. A recentPew study shows that 27 percent of American adults would not get a coronavirus vaccine even though mass inoculation from an effective vaccine would be the surest way to end the crisis—for schools and businesses to reopen, and for people to be able to congregate and resume their normal lives without fear. As Watson had told me, “I do think that vaccine is ultimately the way that this gets resolved.”
During my walk, I came to realize that even in a best-case scenario, the rollout of a mass vaccine campaign will face unique challenges. Even if the logistics of manufacturing enough vaccine to curb a global pandemic are somehow resolved, a mature anti-vaccination movement can undermine its deployment and therefore its effectiveness. Whenever it finally appears, the coronavirus vaccine will test the limits of modern science in a post-truth world.
A nurse evaluates a coronavirus COVID-19 patient in an intensive care unit (ICU).Justin Sullivan/Getty
Holly Valentine, a nurse practitioner in a practice specializing in cosmetic surgery, had not worked in an ICU for four years. But in early March, after hospitals paused most elective surgeries because of the novel coronavirus pandemic, she called her former hospital managerand asked for shifts at Our Lady of the Lake Hospital in Baton Rouge, Louisiana. As the major medical center in the region, Our Lady of the Lake Hospital was bracing for an onslaught of COVID-19 patients from all over the area. “He said I could start tomorrow,” Valentine recalls.
In March and April, as COVID-19 overwhelmed some healthcare systems across the country, hospitals desperately sought additional nurses to serve infected patients. Some, like Our Lady of the Lake, were able to reorganize workers from within their own facilities and pull in local reinforcements like Valentine, bumping pay by $20 an hour for nurses working with infected patients.
Desperate to shore up their staff, other hospitals and healthcare systems hired reinforcements through independent staffing agencies that recruited nurses from all over the country, offered them sometimes breathtaking amounts of money, and sent them to virus hotspots. As this unfolded, the complex, often fragile relationship among medical personnel, healthcare systems, and the staffing companies that sometimes broker the relationships between the two has been stressed like never before.
“Not everybody is going to quit to chase hazard pay,” says Joanne Spetz, a health economist and associate director of research at Healthforce Center at the University of California-San Francisco. But only a handful of nurses need to leave for travel nurse contracts to spike a hospital’s costs, and bumping their pay to maintain their staff has turned out to be a necessary strategy to keep them around. “It may be a better deal to pay the extra money now than the even higher travel nurse rate that you’d have to pay for those who slip out the door.”
When New York City hospitals faced an onslaught of coronavirus patients in March and April, New York City Health and Hospitals, which was responsible for deploying staff to public hospitals throughout the city, expanded its capacity by hiring thousands of travel nurses at often astonishing rates—up to $13,000 a week, more than six times the average pay. Nurses arrived from all over the country to work. Northwell Health, a 23-hospital network that covers New York City and Long Island, and the largest private employer in the state, hired hundreds of short-term travel nurses from staffing agencies to prevent hospitals from being overwhelmed by unprecedented demands. Under normal circumstances, Northwell Health, with a $12 billion annual operating budget, employs 69,000 people—about a quarter of them nurses.
After state governor Andrew Cuomo called for hazard pay in mid-April, some healthcare providers began offering their frontline employees extra benefits. In Northwell Health’s case, some medical workers received a $2,500 pay bump and extra paid time off. But at the same time, rates for travel nurses far exceeded what these hospitals were able to offer their regular staff, which could have posed a potential problem for hospitals hoping to not lose staff to once-in-a-lifetime travel pay.
Under normal circumstances, a travel nurse might replace a hospital staffer who goes on leave, say, for a family emergency or the birth of a child. Staffing agencies are frequently called upon to send nurses to crisis zones when a natural disaster strikes. Sometimes travelers are used for union-busting during work stoppages. Hospitals coping with the demands from the pandemic who turned to staffing agencies needed lots of specialized nurses for lengthy periods of service, while being forced to pay them the high rates usually reserved for short-term deployment. Northwell Health, which hired more than 500 nurses from nurse staffing agencies during the height of the pandemic, anticipates keeping 250 of them on the payroll through June. When I asked Maureen White, chief nurse executive for the network, about the high price tag, she told me, “We believe very strongly that if you do what’s right for the patient, it will be what’s right for your bottom line. And so, we did not look at the bottom line.”
In some parts of the country, where the spread of the coronavirus has been less intense, many nurses have been furloughed by hospitals that had stopped elective procedures. For them, the uncertain economic outlook makes travel nursing and its lucrative pay more attractive than ever. Other healthcare providers are trying to avoid furloughing or terminating their own employees, even though income from elective surgeries remains frozen. Experts on the economics of healthcare see healthcare systems forced into a dangerous guessing game that threatens public health and the solvency of the hospitals trying to provide it.
The best-case scenario for a hospital anticipating a crush of COVID-19 patients would be for it to expand its medical personnel to cover ICU and critical units, either by hiring help or reassigning its existing staff, and then reorienting the space and equipment to increase the number of beds, wards, and medical devices to absorb the new patients. If the local community practiced social distancing and effectively flattened the curve, the hospital would have taken a number of costly steps that proved to be unnecessary. “You’re all dressed up for the prom and the date didn’t show,” is the way Spetz describes it.
In Seattle, the University of Washington Medical Center is an example of that almost best-case scenario. The virus may have first appeared in the US there in late January—though difficulty in tracking leaves scientists and officials uncertain of pinpointing the timing and location. UWMC acted fast, and with a combination of increased healthcare spending and effective quarantining by the community, the severity of the outbreak was contained. The hospital was not overrun by COVID-19 patients, and enough staff was there to provide services. Then came the consequences: Nearly four months after the first cases were reported, on May 18, UWMC announced a $500 million budget shortfall and furloughed 1,500 of its 30,000 employees.
During a press conference announcing the cuts, UW Medicine’s chief health system officer Lisa Brandenburg explained what had happened. First, “we cancelled all elective procedures,” she said. “The second is that we had increased expenses of caring for COVID-19 patients.” Now the hospital plans to return to the elective procedures that had sustained the organization. “I don’t wish trauma or burns or solid organ transplants on anyone, but that’s what these hospitals are built to do,” Dr. John Lynch, medical director of employee health at the university’s Harborview Medical Center, told me. “The way it’s set up financially, we need those patients to do our job, to keep the hospitals viable. It sounds completely morbid, I understand that.”
As Spetz noted, “This thing has absolutely laid open for everyone to see how the hospital financing structures have all of these perverse incentives in it.”
For hospitals that had contracted with nurse staffing agencies to prepare for COVID-19 patients, the hazard pay rates added to the economic burden from the epidemic that’s still unfolding. During the last few months, “we’ve seen a huge shift in demand and migration,” says Martin Vidal, the CEO of Trusted Nurse Staffing, a Buffalo, NY-based travel nurse company. “When you see pay rates at three times what [nurses] normally see, that means our bill rates are the same. Are these hospitals going to be able to pay that?”
Typically, paying for travel nurses isn’t a problem; they’re contracted on an individual and temporary basis. Since the industry emerged in the 1970s, it has grown to encompass almost 100,000 nurses and hundreds of staffing agencies. According to a 2018 survey by the federal government, travelers make up around 2.6 percent of the nursing workforce. In 2012, nurse staffing was estimated to be a $3.6 billion industry with potential growth to $5.3 billion by 2018. Spetz says a combination of factors were already beginning to threaten travel nurse agencies over the last few years: A nationwide nurse shortage was showing signs of improvement, healthcare providers increasingly turned to local resources to avoid agencies’ transaction fees, and disruptive tech start ups began to offer the same service of matching hospitals with nurses for less money. Then COVD-19 revived the hospitals’ need for major reinforcements—fast.
The wide-scale furloughing of nurses in less-affected regions, especially those who work outside of trauma wards, created a large available workforce at just the time when there was an increased need for intensive and clinical nurses in hard-hit regions like New York City and Detroit. It might sound like a problem that solves itself: Nurses are furloughed in some places because procedures were paused as a result of the health care emergency, and that, in turn, created a supply of nurses for hospitals buckling under the strain of new cases because of the health care emergency. But not all nurses have the same skill sets and specialties that hospitals facing overwhelming demands from COVID-19 patients required.
“It’s an imbalance in the whole market,” says Spetz. “This new cohort is looking for travel temp work, and there’s a sudden demand, but the demand is not broad-based. The need is for people comfortable with ventilators, in ICUs and emergency departments. This is a double mismatch.”
Both healthcare providers and staffing agencies have turned to the Joint Commission, a healthcare evaluation organization that credentials both, to assess each other’s quality. For the last decade Northwell Health—one of the 22,000 providers whose facilities the Joint Commission accredits—has relied on Cross Country Nurses, in part because it’s one of the 450 staffing agencies that’s also certified by the Joint Commission. However, on March 16, the commission suspended its evaluation practices, to “allow health care organizations and professionals to focus on preparing and caring for patients with COVID-19,” Joint Commission Maureen Lyons wrote in an email.
In March and April, NYCHH needed still more personnel, despite concerns about a lack of personal protective equipment for healthcare workers. Vidal says he saw hospitals and healthcare systems begin to loosen requirements. “Hospitals were taking in anyone they could,” he says. “They didn’t need OR nurses, they needed anyone with a nursing license, period.”
In early March, Krucial Staffing, a Kansas-based travel nurse company that is not certified by the Joint Commission, contracted with New York City Health and Hospitals and began sending thousands of healthcare workers to hospitals slammed by COVID-19. Krucial was offering three-week contracts of up to $13,000 a week. I asked Julie Aultman, a medical ethicist at Northeast Ohio Medical University, if she’d ever seen similar pay rates in the world of nurse staffing. “The only time I’ve ever seen [rates] like that,” she replied, “is people trying to get college-aged women to donate their ova.”
Some nurses who contracted with Krucial ultimately regretted their decision. Alawsuit filed by seven former Krucial-hired nurses alleges “unsafe” clinical conditions where PPE was unavailable and nurses were asked to perform work beyond their scope of training, endangering themselves and patients. “There’s death and dying everywhere you go. There are no ventilators, no gloves, nothing,” Jose Pinlac, a nurse named in the lawsuit, told me. “It [was] like a war zone.” Another nurse, Mindy Evangelisti, who was contracted with Krucial but isn’t listed in the suit, said, “People were getting thrown into that who had just gotten out of nursing or PA school. So it’s unfair to the individual—and probably to the patients.”
Krucial Staffing did not respond to requests for comment on this story.
When Valentine arrived for work at Our Lady of the Lake in Baton Rouge, the hospital had converted three floors into a mass ICU to accommodate more than 250 seriously ill COVID-19 patients, many on ventilators; the pediatric unit was converted for those in recovery. Orthopedic, operating room, or recovery ward nurses in the hospital were moved to the trauma floors. In some cases, ICU nurses were paired with those pulled from other specialties, operating in small teams, to ensure things ran smoothly. “This was a total seat of the pants situation—out of necessity,” she says. By the end of April, the patient surge had subsided.
New York City found itself on a similar timeline. On May 19, thecity reported 993 new cases, down from more than 3,700 two months earlier. The Krucial Facebook page, from which the company once broadcasted recruitment ads for hundreds of nurses at a time, is now dominated by posts celebrating the heroism of nurses. “Looking back, what are some of your favorite memories on deployment?” one post asks followers.
COVID-19, however, isn’t over. To make up for lost time, hospitals are beginning to resume the elective surgeries that provide essential income. With public health experts predicting potentially more devastating waves of the pandemic in the fall, there’s not a moment to lose.
“So now we’ve bought some time,” says Spetz. With it, she says, the industry of healthcare can start to reshape itself in preparation for the next surge—whether its COVID-19 or something else. The recent experience of this epidemic, however, has forced health care institutions to face a key question: Should they find the most efficient way to import travelers with ICU experience, or build a more flexible network from within their own personnel rosters, which might result in reducing travel nursing into a much smaller operation? “That’s a debate that’s above my pay grade,” she says.
The artist Jorge Rodríguez Gerada with a portrait of Dr. Ydelfonso Decoo, an immigrant doctor who died of complications from coronavirus.Pablo Monsalve/Getty
In early March, Dr. Karanjit Sandhu, a hospitalist at the Albert Einstein Medical Center in Philadelphia, contracted the coronavirus from a patient. He worried how the virus would affect his body and whether he’d recover. Yet as he spent two weeks in bed with a fever, aches, and extreme fatigue, another concern was hanging over his head: How the illness might affect his family’s immigration status. “If for some reason I couldn’t work and I had to leave my job, we don’t really have a legal status,” he says. “It’s just an unknown, and obviously that created a lot of anxiety on top of being sick.”
“As morbid as it sounds, it’s something we had to eventually think about and prepare for,” says Dr. Bhavna Sharma, who is married to Sandhu and works as a pulmonologist, sleep therapist, and intensive care unit physician at the same hospital. She recalls the two weeks when her husband was battling COVID-19 as one of the most stressful moments of her life. She started preparing for worst-case scenarios in which he became permanently disabled or did not recover at all. If he had died, Sharma says, “Not only do I lose my husband but potentially also lose my job and also have to leave the country within 30 days, move my kids and leave everything behind. So that was definitely a real fear.”
Sandhu, who is from India, has an H-1B, a temporary work visa that’s held by more than 400,000 highly educated workers including doctors, engineers, and researchers. Nearly three-quarters of H-1B visa holders are from India. Sandhu and his family can live in the United States only as long as he is able to work for his employer. (Sharma has an H-4 visa, issued to the spouses and children of H-1B holders.)
Immigrant doctors such as Sandhu and Sharma are on the frontlines of the coronavirus pandemic, often treating underserved communities that have been hit disproportionately by the disease. At a moment when their work has never been more essential, more of these doctors are speaking out about the rules that leave them and their families without a safety net if they get sick and also make it harder for them to contribute to the fight against COVID-19. With help from advocates and allies in Congress, they are pushing to speed up the sometimes decades-long process of obtaining permanent residency. “You have all of these physicians putting their life on the line. And now they have to wait 20 years to get their green card? There needs to be something to help them out,” says Mahsa Khanbabai, an immigration attorney and the chair of the New England chapter of the American Immigration Lawyers Association.
Dr. Karanjit Sandhu and Dr. Bhavna Sharma with their two children.
Credit: Dr. Bhavna Sharma
Dr. Sujit Vakkalanka is a hospitalist in Galax, a town of around 7,000 people in the mountains of southwestern Virginia. Twin County Regional Healthcare, where he works, serves two nearby counties and is the only hospital in a 30-mile radius. If he wants to shop for Indian groceries or watch an Indian movie, he has to travel 100 miles to Charlotte, North Carolina.One in five practicing physicians in the United States is an immigrant. According to a survey conducted by the advocacy group Physicians for American Healthcare Access, nearly half of the physicians serving areas where the per capita income is below $15,000 a year are immigrants.
Vakkalanka’s schedule consists of working for one week and taking one week off. He would like to use his off week to help out at hospitals facing a shortage of doctors. He has a license to practice in New York, and Gov. Andrew Cuomo’s office has contacted him several times asking him to help. But he can’t add a new employer unless without getting a new H-1B, which could take months. “The process is very burdensome and there’s a lot of red tapeism,” Vakkalanka says. “Even if we’re willing to go and help, we’re unable to do it.”
The H-1B visa was created as part of the 1990 Immigration Act to bring skilled workers into the United States. It’s a three-year visa; if an employer sponsors a visa holder worker for permanent residency, they can get unlimited three-year extensions until they get their green card, a prerequisite for obtaining citizenship. Thousands of H-1B holders qualify for green cards every year, yet there’s a cap on how many green cards can be issued to each nationality. As of May 2018, nearly 600,000 H-1B workers and their families were waiting for employment-based green cards. More than 90 percent are Indians, who receive about 10,000 employment-based green cards a year. The green card backlog is daunting: the CATO Institute, a libertarian think tank, estimates the wait time for Indians with advanced degrees is 49 years.
Most people in the line for green cards are tech workers, but there 12,000 physicians on the list, according to estimates from Physicians for American Healthcare Access, which is lobbying for green cards for immigrant doctors, primarily from India.
Frontline doctors on H-1Bs are hopeful about a new bipartisan bill that could streamline their path toward residency. The Healthcare Workforce Resilience Act, introduced by Senators David Perdue (R-Ga.), Dick Durbin (D-Ill.), Todd Young (R-Ind.), Chris Coons (D-Del.), John Cornyn (R-Texas), and Patrick Leahy (D-Vt.), would immediately give unused green cards to around 15,000 doctors and 25,000 nurses who are currently in the backlog. “Consider this: one-sixth of our health care workforce is foreign-born,” Durbin said in a press release in late April. “It is unacceptable that thousands of doctors currently working in the U.S. on temporary visas are stuck in the green card backlog, putting their futures in jeopardy and limiting their ability to contribute to the fight against COVID-19.”
Khanbabai, the immigration attorney, notes that many doctors waiting for green cards have dependent kids who could lose their H-4 visas and be deported when they turn 21. That’s what happened to Dr. Preeti Saran, a primary care physician at the Robert Wood Johnson Medical Group, part of Rutgers University in New Jersey. Saran came to the United States in 2002 with her then-12-year-old son. When her son turned 21 he had to go back to India. “How could they not honor someone who has served the country for so long?” asks Saran, who has been waiting for a green card since 2010. “We are not asking for anything other than our status because that can allow us to serve better.” Recently, her son moved back to the United States to pursue graduate studies. But he’s looking for jobs in Canada, and Saran is considering moving there with him.
Like Saran, Sandhu has been stuck in the green card queue for around a decade. He has been working on an H-1B since 2007; his employer sponsored his green card petition in 2010. Most of his colleagues from other countries have already become naturalized citizens. During this time, he and his wife couldn’t pursue fellowships to advance their careers because they can’t change employers easily.
The long wait has started wearing them down. “It’s been the biggest source of anxiety,” he says. “And just the uncertainty, it’s just unrelenting. You have to juggle so many issues just because you’re on a visa, I think, that itself creates chronic anxiety,” he said. It’s “just kind of disappointing that, you know, 10 years down the road, we’re still in the same boat.”
After spending two weeks in isolation after he was infected with COVID-19, Sandhu applied for a National Interest Waiver green card, which is open to physicians who agree to spend five years working in hospitals treating underserved communities. With his seven years of experience working in low-income communities in Philadelphia, he thought he’d qualify. Einstein serves a federally designated “medically underserved area” in North Philadelphia, where nearly a third of the population makes less than $25,000 a year and nearly half the population is Black. As in other cities around the country, COVID-19 is disproportionately affecting Black people in Philadelphia, who account for around 44 percent of the city’s population but 51 percent of its coronavirus fatalities.
If Sandhu was approved, he wouldn’t get a green card immediately, but he would have more flexibility in changing employers or pursuing a new specialty. (He would like to pursue a prestigious fellowship in cardiology within Einstein.) His application to United States Citizenship and Immigration Services required an approval letter from the state of Pennsylvania. But the state’s department of health refused to give its approval, telling him that his past experience at Einstein wouldn’t count toward a National Interest Waiver.
“We have made it our policy not to entertain prior service requests because of the time needed to collect and review five years of documents to ensure compliance with the program, for a physician with whom we had no prior relationship,” said Nate Wardle, spokesperson for the Pennsylvania Department of Health in an email. States have different sets of criteria for which doctors qualify for a National Interest Waiver. Some, including Florida, Georgia, and Illinois, accept doctors’ past experience to count towards the requirement.
The Healthcare Workforce Resilience Act recommends that all states change their National Interest Waiver policies to support the green card application of any physician who has worked for an underserved community for five years. Khanbabai says that considering doctors for permanent residency based on their experience in underserved communities will help states attract doctors, especially since they’re facing a shortage. (Estimates from the Association of American Medical Colleges indicate that the United States could have a shortfall of between 21,000 and 55,000 primary care doctors by 2023.) “Physicians deserve to be acknowledged for their prior work in communities which often have a very difficult time recruiting health care providers,” she says.
There’s no date set for a committee hearing on the bill, but physicians who are part of Physicians for American Healthcare Access are hoping it might pass as a part of the next coronavirus stimulus package. “It’d be a welcome relief if they could pass [the bill],” Sandhu says. “It’d be a godsend. That move would solve a lot of the problems that immigrant physicians are facing. There’re so many of us, who want to contribute to the American society, want to raise their families, live here. I think it’d just be a win-win for everybody.”
West Point did not need to have an in-person graduation ceremony this year. The nation’s oldest military service academy had its cadets leave campus in March as the coronavirus outbreak began spreading across the United States, especially in New York, which has more than twice the amount of infections as any other state.
But President Donald Trump insisted on giving an in-person speech to the 1,000-person graduating class for the June 13 commencement, forcing Army leaders to scramble their plans and summon cadets back to campus. On Monday, the Army completed a screening of all returning graduates and announced that 1.5 percent, about 15 or 16 students, had tested positive for COVID-19.
“This was anticipated,” Army spokesperson Emanuel L. Ortiz said in an emailed statement. “None were symptomatic, and no cadet has contracted through person-to-person contact while under the Army’s care.”
Even if a few positive tests were inevitable, Trump’s insistence on speaking in person was not. In March, as West Point leaders discussed whether to return students currently on spring break to campus, Trump abruptly announced his intention to attend the ceremony. The New York Times reported that academy officials “were taken aback by the impromptu announcement” and were forced to improvise after Trump “preempted their planning.”
There is no reason for Trump to gather the cadets in person for a commencement address. Secretary of Defense Mark Esper addressed Naval Academy graduates virtually last month and even the Air Force Academy, which controversially kept seniors on campus during the outbreak, welcomed Vice President Mike Pence for a commencement event where social distancing protocols were in effect and zero spectators could attend.
Trump evidently expects a similar ceremony with more pageantry at West Point, the only service academy he has not yet addressed as commencement speaker. In April, he told reporters that he assumes the academy will “have distancing” at the event, unlike the “nice and tight” commencements of years past.
Presidents from Theodore Roosevelt to John F. Kennedy have traveled to West Point to speak at commencement, and Trump is not one to forgo the pageantry of a commander in chief addressing his troops. Lt. Gen. Darryl Williams, the academy’s superintendent, told reporters at the Pentagon that returning cadets will be “segregated the entire time” into five cohorts and no cohort will intermingle for 14 days. “They’ll eat separately, they’ll live separately,” he said.
The Army has struggled to justify Trump’s decision, which requires hundreds of future soldiers to return to a region of the country that has been hit especially hard by the coronavirus. Ryan McCarthy, the Army’s top civilian leader, said cadets would have needed to return to campus anyway “to begin the process of the physicals they need, to take all of their clearance procedures, to clear barracks, get their personal items.” But that process could have been spaced out in a way that would have ensured greater safety for cadets. Even academy alumni and parents were reportedly stunned by the decision. “There is no military need to do this,” Jason Fritz, a 2002 West Point graduate, told the Washington Post. “This is a logistics nightmare, all just so the president has an audience to give a speech he wants to give.”
The commencement speech has sparked an uproar on the West Point Parents Facebook group, where most posts tend to be anodyne calls for support for cadets and the Army. In a thread announcing Trump as the graduation speaker that appeared in April, when the decision was announced, several posters blasted the decision as both narcissistic and dangerous. “PLEASE PLEASE do NOT let your children go back for graduation. It’s not worth their health or yours,” one person wrote. But others contextualized Trump’s mandate by comparing it to a typical order from a commander in chief, including ones that send cadets off to war. “For those who have not yet done so, use this time of social distancing to come to terms with the choice our children have made,” another parent suggested, “and realize that this choice will likely put them in harm’s way in some way, shape or form.” Including on graduation day.
The University of Connecticut shut down its campuses on March 12, 2020.Dennis Tangney Jr/GETTY
As seniors graduate from high school and wonder about September, and parents enter their third month of homeschooling following coronavirus closures, two questions seem to preoccupy everyone: When will schools open, and what will they look like when they do?
On the Mother Jones Slack channels, data has been considered, theories posited, and lots of questions asked. Could schools hold classes outside? What’s the incidence of coronavirus infection in children? How will this impact decisions to reopen schools? Which universities are doing what to plan for the fall? Our reporter Kara Voght often offered key insights in these discussions, partly because she covered education before politics, but also because she has a trusted inside source. Her mom, Donna Korbel, is assistant vice president for students affairs and the director of the Center for Student Disabilities at the University of Connecticut (UConn), where she’s worked for the past 27 years. Without disparaging her journalist daughter’s professional choices, Korbel likes to joke that she doesn’t understand why anyone would want to work anywhere without a marching band.
The University of Connecticut, a public research university, serves more than 19,000 undergraduate students. Seventy-five percent of those students live together on campus in classic dorms where everything is shared. The campus is at the heart of the college experience at a school like UConn, which has a student population the size of a small town. But like colleges and universities across the United States, when the coronavirus outbreak hit, UConn shut down its campus, sent students home, and took classes online. For the past few months, Korbel and her fellow administrators have been trying to figure out how they can safely reopen the campus.
Since we’re both working from home and social distancing, I caught up with her via Zoom to get an inside look at how university administrators are thinking about reopening their campuses. This is what she had to say, edited for length and clarity:
On the hazards of communal living
We know our students want to come back to campus. This is not the college experience that they signed up for. But we have to be concerned with health and safety. When you think about reopening an overwhelmingly residential campus, and look at the social distancing requirements that are in place, and the recommendations for testing—it’s complicated. Many of our residence halls are over 50 years old, and they were built at a time when there was an emphasis on communal living. You had a roommate, you shared a bathroom, you share a living space, and all of that flies in the face of what’s appropriate in a COVID-19 environment.
I’ve worked in student affairs now for 40 years and I’m all about the student experience. Thinking about that student experience, there are all the operational questions: How to feed them? We can’t have dining halls open, so it’s takeout. Well, where will they eat? Are we expecting that students will pick up their meals and go back to their rooms by themselves and eat? That’s just not behavior consistent with everything I know about somebody between the ages of 17 and 24.
On when UConn will reopen
Many schools have made their decisions about the fall already. We’re not going to make ours until June. UConn is between New York and Boston. New York and Boston are hotspots for the disease. We have a campus in Stamford, which is 20 minutes outside of New York City, the epicenter of the disease. We’re not going to take any chances. We will do this with an abundance of caution with the best information that we possibly can. We know that at least part of our instruction will need to be online for the fall, just based on social distancing necessities.
We are very much working off the guidance of our governor, Ned Lamont, and the higher-education COVID task force. We’re an outlier in Connecticut because we are such a large residential campus. But some of the guidelines remain the same in terms of monitoring, testing, containment, quarantine. How do you plan for keeping students, faculty and staff, safe? How can you safely house them? Can you bring them all back? Should you only bring back 50 percent? Even if you bring back 50 percent, how do you make that decision? There are lots of moving parts and just so many questions the issues around the availability of the kinds of testing equipment that we’ll need, and the monitoring.
On minimum testing requirements for reopening
Everyone would need to be tested. There’s not a different standard for faculty, students, or staff. Everyone would need to be testedcoming onto campus—details to be determined but most likely when they get to campus—and would that be repeated like somewhat regularly. The guidelines also call for us having a place where people can be safely quarantined.
On scenarios that administrators are considering
We have several different models that we’re looking at. As a university we always have committees, right? We have academic committees, we have student life committees, we have the facilities committee looking at capacity of classrooms.
For a university our size, we don’t really have lots of large lecture halls. That’s always been a big strength of UConn, and students have really appreciated that we don’t have the kind of big lecture halls that you ordinarily expect at a Research I. Nonetheless, even with a classroom of 70 seats, or 35 seats, you don’t have that capacity anymore when you have to see people six feet apart. So the Facilities Committee is working on coming up with a new capacity is for classrooms—maybe repurposing the dining halls? Dining halls are very difficult for social distancing, even in terms of meal prep. Our dining halls weren’t designed so that people could stand six feet apart while either serving or preparing foods. So just looking at every possible scenario in terms of how we think about space differently.
On the idea of a staggered opening, where first-years and juniors are on campus from September to October, sophomores and juniors from November to December
That was a model that we looked at. Our medical folks looked at that and said, it’s difficult for us to think about every couple of weeks bringing new people to campus who would have to self-quarantine for 14 days. You really would need to self-quarantine. Seventy percent of our students come from Connecticut, and for the rest we draw a lot from New Jersey New York. The staggered [opening] may work for some campuses. We have to talk about the scale at UConn.
On technology requirements for an online education
Yesterday, I was on a call with the group where we’re talking about technology. It’s an equity issue. When you move to an online environment, you can’t make assumptions that everyone has a state-of-the-art laptop or desktop and high speed internet and smartphones. We certainly found that that wasn’t the case. So we’ve been reaching out to students and trying to provide assistance through our Students First Fund. Our IT departments scrambled to find every laptop and iPad that was available on campus. Just so many issues. In the spring semester, we had to do a quick pivot and do the best we could.
On students with unique learning accommodations
We work with over 4,300 students with disabilities. Each semester, students are evaluated based on their coursework and what their accommodation needs are. Some students may opt not to come back to campus because they’re in a compromised situation. We have students who are receiving treatment for cancer. We have students who have autoimmune conditions. Students will not be denied the opportunity to study online.
The primary population of students that we work with are students who have psychiatric disabilities. This is a very difficult time for people, for all of us. Feelings of loneliness and trying to adjust to this is just a very different experience. Students are having difficulty engaging in therapy because, in some cases, their family members didn’t know they were in therapy. It feels very different to be talking about things with your therapist when you’re at home. They don’t feel particularly private in their home, even if they have a private space. And we’re very aware that not everybody has a home to go to. So when students left campus, we had about 1,200 students that for whatever reason—whether they were international students or just didn’t have situations where they feel they could return to—they were allowed to stay on campus until the end of the semester.
On the possibility of being sued if campus reopens and students get sick
That’s a national issue that every college is grappling with and thinking about. We will be making a decision locally, but we will be following the best advice that’s out there. Our president has been very, very, clear about that. I always joke about academia, we are the people who still wear clothes from the Renaissance. So we tend to be pretty stable. We are certainly going about this in a very thoughtful and purposeful way.
On how the coronavirus is affecting enrollment for the 2020–2021 school year
Our enrollment numbers are up. When we say enrollment numbers, that means deposits. Students needed to make that commitment by May 1. Some colleges pushed that deadline out, we did not. UConn is a very popular brand. So we have a robust number of students who indicate that they want to come, but we also know that it depends what September looks like. Students may opt to take a gap year, or just opt to stay closer to home. There’s so many things, and we’re aware of that. Every decision we make will affect actual enrollments for fall.
On whether she’s ever seen anything like this in her 40 years of working in student affairs
No. There isn’t even anything that comes comes close. We missed all the end-of-the-year celebrations. We had a YouTube graduation, and we’re hoping to have a ceremony in October. All of those things are just extremely difficult because they’re very personal.
On her favorite part of her job
Oh, students. Interacting with students, working with students, being on a college campus. There is just something remarkable about watching the transformation of students. I started my career as a rehabilitation counselor. My whole philosophy of rehabilitation is that you create an environment where people can become as independent as possible. UConn has remarkable opportunities for students with disabilities. To be able to work where I can facilitate the environment for people to achieve maximum independence, I just feel like I’m one of the luckiest people in the world. I had the good fortune to do this work in a place I love.
Closing thoughts
We miss students as much as they miss us. We are being so thoughtful and so deliberate about not only making sure that we give them the best possible experience that we can, but also that we do it safely. Part of the role of a great university is to produce citizens. The way that you do that, lots of times, is through your co-curricular activities. We understand that students will remember lots of things about their college experience. They’ll remember their freshman English class. But most often they’ll remember the clubs and organizations, the parties, the conversations they had in the residence halls, the dining halls, going to a sporting event. We are very cognizant of that. We want to make sure you know we want to bring them back as soon as we can as safely as we can, and give them all the things they’re missing.
Pastor Brain Herron helped pass out masks to North Minneapolis residents in April.Jerry Holt/Getty
As residents of Minneapolis mourn and protest the death of George Floyd, the city’s Black community is also reeling from the coronavirus. Just as Floyd’s killing by a white police officer has resurfaced the effects of structural racism, the virus’ disproportionate impact has highlighted the lack of equitable healthcare access and other risk factors that have made African Americans more vulnerable to COVID-19.
As we have reported, in many states, Black Americans’ rates of infection and death have been much higher than their share of the population. Similarly, Minneapolis’ Black population has been disproportionately infected by the coronavirus. As of May 29, 34 percent of people who were infected with the virus in the city were Black, though only 18 percent of the city’s population is Black. While the city’s population is 64 percent white, 24 percent of those infected with the virus were white.
So far, 5,361 Black people have been infected by the virus in Minnesota. Minneapolis is one of six cities in the country where more than 10 percent of test results have come back as positive, according to White House Coronavirus Task Force Coordinator Dr. Deborah Birx.
Commenting on the fires lit during last night’s protests, Minnesota Gov. Tim Walz (D) said, “The ashes are symbolic of decades and generations of pain, of anguish.” The statistics above are another sign of the pain that continues to go untreated.
As quickly as scientists are working to develop a vaccine for COVID-19, there’s a plethora of companies working just as fast trying to illegally profit from the novel coronavirus, mostly through fraudulent treatments, bogus tests, and various other scams. Though there isn’t currently a vaccine or a largely effective treatment for COVID-19 , as the Centers for Disease Control has repeatedly emphasized, that has not stopped a growing number of companies from fraudulently claiming that the products they sell contain certain substances—like colloidal silver, kratom, CBD oil, and even bovine colostrum— that can treat or prevent the virus. And while the Food & Drug Administration and the Federal Trade Commission have focused their efforts on cracking down on COVID-19-related fraud, the scams continue to flourish.
According to the FTC’s own data, as of May 27 there’s been more than 55,000 consumer complaints related to COVID-19, with 31,000 of those complaints specifically related to fraud. In all, the FTC has reported that people who fell victim to a coronavirus-related scams have lost at least $40.39 million. Though the agency has reported thousands of instances of fraud in the form of identity theft and robocall scams, most of the COVID-19-related complaints that the agency has received have been related to travel scams, text message scams, and online shopping—particularly as it relates to products sold online that make false claims about its effectiveness in treating or testing for COVID-19.
In one recent case, a California-based company called The Golden Road Kratom claimed that capsules of kratom—a controversial though currently legal drug that advocates say can treat a laundry list of ailments, including opioid withdrawal—were effective for both treating and preventing COVID-19. According to a warning letter sent by the FDA, the company had falsely stated on its website that kratom “contains a special compound known as chloroquine…that research shows is powerfully combative against the coronavirus,” and that Wuhan-based researchers said that “chloroquine can be used for the treatment of patients with Covid 19.” The company no longer has these claims on its website.
In a press release sent last week after the FTC reported receiving 50,000 COVID-19 fraud complaints, public interest advocacy group US PIRG called it a “dubious milestone.” “We see this sort of thing after natural disasters and economic crisis, and you kind of have both happening right now,” says Mike Litt, who directs PIRG’s campaign to defend the FTC. “COVID-19 has changed every aspect of our lives, so there are countless ways for people to be scammed. People are cooped up at home, scared about their finances and their health. And scammers are taking advantage of that.”
Since COVID-19 evolved into a full-blown pandemic, PIRG has been tracking the federal response to coronavirus fraud. Thus far, the FTC has sent out more than 150 warning letters to companies, suspended the stock trading for 30 companies, and has shuttered thousands of web domains and email addresses. The Department of Justice, meanwhile, has taken legal action in nearly 20 instances of coronavirus-related fraud. And US Immigration and Customs Enforcement launched an operation in mid-April, which the agency says has led to 458 coronavirus-related seizures, totaling more than $3.2 million in illicit proceeds seized. Most recently, the agency seized nearly 6,000 fraudulent COVID-19 test kits and thousands of pills purported to treat the coronavirus, including pills claiming to be Hydroxycloroquine Sulfate, in Buffalo.
Still, even with a number of federal agencies diverting their resources specifically to combat COVID-19-related fraud, Litt says it’s hard to assess how effective their efforts are. In the case of the FTC, Litt says the agency should publicly report the responses it receives to warning letters, similar to what the FDA is doing. In the FDA’s database of warning letters, it includes a column for the response from each individual company, to indicate if that company responded to the FDA’s letter and if it actually led to a cessation of sale of the fraudulent product.
Despite that, the sheer quantity of products flooding the market has allowed some to fly under the agency’s radar. While analyzing the myriad fake COVID-19 products online, PIRG found several examples of products claiming to treat COVID-19 that the FDA had not warned. One brand that PIRG flagged, 78Minerals, sells nutrients and minerals that it claims will “[help] fight coronavirus and strengthen your immune system.” The FDA has not issued the company a letter warning them to stop marketing their product as a COVID-19 treatment, according to a search of the agency’s warning letter database.
And some lawmakers think there’s more that can be done than just sending out warning letters to address COVID-19 fraud. Earlier this month, Senate Minority Leader Chuck Schumer (D-N.Y.) called on the FTC to crack down harder on coronavirus scammers, asking the agency to issue heavy fines rather than just sending out warning letters. “Let’s face it, there are a lot of older people, there are a lot of just average folks who are desperate,” Schumer said. “These scammers prey on people in their weakest moments.”
Mortician Cordarial O. Holloway, foreground left, funeral director Robert L. Albritten, foreground right, and funeral attendants Eddie Keith, background left, and Ronald Costello place a casket into a hearse on April 18, 2020, in Dawson, Ga. AP Photo/Brynn Anderson
As of Wednesday afternoon, the United States as an official matter had lost 100,000 people to the coronavirus—100,000 people who are irreplaceable to someone else. This threshold was crossed without the large-scale acts of public mourning with which we typically observe mass death. The closest thing to it was the sobering front page of Sunday’s New York Times, which listed the names of 1,000 people who’d died of COVID-19 in the United States.
Earlier this week I called up Dr. Kami Fletcher, wondering if and how Americans were processing so much death in their midst. Fletcher is a historian at Albright College, co-author of Till Death Do Us Part: American Ethnic Cemeteries as Borders Uncrossed, and president of The Collective for Radical Death Studies, which works “to analyze how death, mourning, burial, and death investigations have changed over time along the lines of race, class, gender, ability/disability, sexuality.” Her work centers on the ways that asymmetries in life persist in death—a subject particularly relevant to a disease that has taken a heavy toll on Black and Latinx people.
Fletcher and I spoke about the “death-denial culture” in the United States, the disruptions caused by the coronavirus to Black death rituals, and how the country would be mourning today if the pandemic were disproportionately killing white people. Our conversation has been edited for clarity.
I wanted to start by asking about the cover of the New York Times over the weekend. I’m curious to hear what was going through your mind when you saw that.
A good historian friend of mine shared a similar thing from the Spanish flu of 1918, and looking at the New York Times front page, it brings humanity to it. These were people, these were living, breathing people. They were part of our educational system, our job network here. These were Americans. These were people who have left behind family members who are mourning, who are grieving, and who have unanswered questions. Let’s start having a real human connection to this.
I’ve been thinking about the idea of not being physically together at a time of mourning. We can’t get on a plane or a bus or a train, and travel to be with our families after a loss. We can’t console each other. That physical distance adds to the anxiety that builds up when you’re cooped up at home, knowing something has happened and you can’t be there. What does that do to how we process death?
We’re in a death-denial culture, as Americans—we deny death. That’s really the prevailing idea. We put death in a hospital, we put death in a hospice, and we try to have a quick funeral, and it’s private. We try our best to deal with it and go on. Which is the complete opposite of what Black folks have been doing. Black people and people of color who have been dealing with white supremacy, with racism, and with the legacy of direct colonial rule have had to adjust and adapt. And it shows in our mourning customs.
I just want to make a point here. There was a 7-year-old girl [Jakelin Caal Maquin from Guatemala] who died two years ago [in Border Patrol custody] and while unfortunately it’s not an irregular story, it made news. And I remember posting that on Twitter and saying that whatever mourning rituals were happening were to try to explain why the 7-year-old girl is not here anymore. That’s what death rituals do. That’s what mourning is about. And right now, we cannot group, we cannot sit with the bereaved.
There’s no way that we can talk about deaths from the coronavirus and not talk about race. People of color are being hit particularly hard by the virus. As a Mexican immigrant, I think about how this affects my community. So how does the African American community grieve right now? Is there collective grieving within a community when it’s so hard to grieve in general?
The color of COVID is Black and Brown, I think it’s very clear. Every person that has died of COVID in Richmond, Virginia, was Black [as of mid-April]. We’re also talking about Native Americans—the Indigenous population in certain areas of the country are just being decimated. And some of the reasons why are just bureaucracy. They literally cannot get the funding to the groups of people.
Which goes back to your question about why we are not public mourning. It’s because of the mentality of “Black and Brown people just kind of brought it on themselves.” That’s why you cannot talk about death if you’re not talking about culture and history. I’m not even taking into account the different religions or atheists—when I talk about Black folks, I’m talking about this collective Black experience born out of slavery and oppression. So are our funerals going to be three or four hours? Absolutely. Absolutely. Because to mainstream society we’re just a number: “Oh a bunch of Black people died, they had high blood pressure already, they smoked a lot, they drank a lot.” There’s no care. There’s no concern there.
But at the funeral, that was somebody’s daughter. That was somebody’s mother. She actually served as the president of the PTA. She actually developed a type of Meals on Wheels program for the elderly in her community. At the funeral, you get this three-dimensional, non-stereotypical image of Black folks in our last-rites rituals. And that’s very important. It’s communal, and COVID has definitely disrupted that.
At the risk of asking the very obvious, what would our collective mourning as a country look like if the faces of those who died were not mostly people of color? If this had been something that really hit white rural America hard? Would we, as a country, our elected officials and our news media, be talking about these deaths differently?
I really am glad that you asked that because I think that lends itself to part of the conversation that we think we know, but maybe we don’t. And we need to have a conversation about it. I think when you’re talking about African Americans specifically in this country, there is a connection to violence and death that people have taken for granted and are okay with. People really think that Black bodies are disposable. White people are authority figures. That’s what white supremacy sets up.
We can draw similarities with heroin and crack. When crack hit Black America, it was about Black people smoking crack and killing each other. But when the heroin epidemic started, it was about opening up centers to help these people. I think everybody should be helped—I don’t want anybody to hear this and think otherwise. Everybody needs to be helped. But it’s been racialized.
I keep hearing stories, reading reports, and seeing in social media that Black people are going to the hospital during this time period and not being believed. They’re being turned away and mistreated. That’s what we’re dying of. And that has to be part of the discussion. You’ve had medical professionals not believing that Black women are in pain, dying in childbirth. I don’t know if people really understand how much they lead with stereotypes.
It seems that—at least for me—that in the beginning of all of this we were hearing more about the dead: a profile of a family, a group of friends at a nursing home, the story of multiple relatives who died from COVID-19. As the numbers kept multiplying, we went to tens of thousands. Do we process that slow day-by-day death count differently than, let’s say, a plane crash or mass shooting or natural disaster that kills many people at once? Is there a difference in how we process this loss?
The first thing is the idea of death and disaster: A hurricane that we cannot control has killed people, or a bomb has been dropped in a war. Is it a difference in how we mourn? I think you have to look at who’s controlling the conversation. When you have a conversation where the surgeon general is saying, ‘These folks are bringing it on themselves, you know, lay off the tobacco, lay off the alcohol,” I definitely think you lose empathy. And there’s distractions going on. I never would have thought—but I guess as a historian I should have known—that these “liberate the state” rallies would pop up. I literally walked out of my house three days ago going to the post office that’s a block from my house and the local courthouse, and I was just shocked and really alarmed and fearful of a “liberate the state” rally. You can’t have people mourning and grieving and feeling sad if you honestly are saying, “No, no, nothing’s really happening here, I’m willing to die of COVID for the economy, let’s sacrifice the elderly.” This is disrupting the kind of national mourning that we should be having when 100,000 Americans are dying.
That closeness that we talked about earlier—I can’t even imagine not being physical in a time of loss, as a Latina, the hugging, kissing, handholding, sitting side by side with someone is so important for us. This makes me think of the public vigils after mass shootings. I’ve been to a few, unfortunately, as a reporter—most recently the one in El Paso where so many Mexican people were killed—and there’s something to be said for having physical space to bring a balloon or a sign, even if you didn’t know anybody who died, just to sit there with a physical representation of death and loss. Those are things we can’t have right now. Do you think something like the New York Times front page shook that back into the conversation a little?
Yeah, I love that “shook that back into the conversation,” because what do you do if you’re trying to flatten the curve? Right now we can’t do a memorial, we can’t take a balloon anywhere. When you look at how African Americans and Latino culture have used the “Rest in Peace” T-shirt, I think that can be a powerful memorial.
Once again this is one of those things that’s been misunderstood because you have this dead person on a T-shirt and you’re walking around with it. People associate it with gang-related activity. So again that’s that kind of deviant, at least what sociologists call “deviant”—not as in devilish, but as in outside mainstream culture. It is a way to memorialize someone by socially distancing too, because what we’re really saying is that these people existed. They lived, they were here, and that’s why you have something like the ghost bike where a cyclist has died. It’s bolted down in a certain place to say this person mattered, something happened here, and we need to address it.
An occasional series about stuff that’s getting us through a pandemic. More here.
It turns out, living through a pandemic inspires a sweaty pressure to Be Productive while real life is on pause, despite also igniting paralytic existentialism that dulls the mind into a neverending loop of sad, gray fuzz. For my job, I have to keep up with a news cycle that is utter chaos. I have a book to report out and research and write. There are so many bread recipes on the internet right now. (Do not talk to me about how William Shakespeare wrote King Lear in quarantine, you shit-talking performance artist.)
This is how I have fallen into obsessively Googling “#studyblr” and sinking into a comforting scroll through Tumblr blogs that host thousands of images, set against pastel, washed-out backgrounds, that look more or less exactly the same.
There is usually a steaming cup of coffee or matcha in the foreground, or maybe it’s a glass of cold brew coffee with an artful swirl of oat milk, all caffeine is welcome here. The beverage is situated alongside a MacBook that displays either the time or the date in a ridiculously large font or maybe some sort of document. Perhaps there’s an iPad with notes that were carefully created using an app and a stylus (that I cannot fathom using in my day.) Or there’s a notebook, open to a page with notes in impossibly beautiful handwriting—headings and subheadings in calligraphy! Colorful little diagrams that look like they sprang onto the page directly from a textbook designed by and for millennials! Highlighters whose neon hues denote categories! A handful of accessories are carefully arranged—nay, scattered—on the desk: Muji pens, the aforementioned highlighters, AirPods, a plant, maybe. There are little messages urging the reader to remember to hydrate, move, and be gentle with oneself.
It’s productivity porn. It’s a completely unrealistic, cozy myth, that the right pair of wool socks and caffeinated beverages can make me Get Shit Done. To be sure, we are in a global pandemic, and the added layer of pressure to use this time (lol) to do stuff is straight out of Capitalism 101 and very worthy of critique. But in this moment, when I desperately crave order and predictability, the mere idea of being productive is a lifeline. If these blogs say I must, then I must.
Let’s face it, I was already susceptible to this sort of propaganda. I grew up stanning Hermione Granger. I am a devoted user of a very specific notebook brand (dot grid til I die). I have spent my life in search of the perfect pen that I now believe to be, yes, the 0.38 mm gel Muji pen, and I do carry that one Madewell tote. I read The Cut’s “How I Get It Done” series with religious regularity, as if by studying the habits of such women as those profiled on my favorite website, I can absorb them into my much messier state of being and become the sort of person who wakes up at 5 a.m. and sips hot lemon water before doing an hour of yoga and then catching up on emails.
Nowhere has this desire manifested itself more clearly than in my book research in my off-hours. It begins with careful reading and highlighting and note-taking. There is tea; I have lists. But it quickly devolves into my usual scribbles in my notebook and in the margins of academic tomes. My tea, largely forgotten, turns cold, my messy bun begins to increasingly resemble the kind of mess a rodent would feel at home in, and I move back and forth from my ink-stained (yes, I fell asleep on my Muji pen once, but only once!!), tangled bedsheets to my “standing desk”—an old, beat up dresser that is on its second generation of Andrews. I’ll never be #studyblr, and that’s really fine. I know I can’t expect myself to be extremely busy and very productive when I’ve been stuck in my house for more than two months away from the people I love and the routine that I’ve carefully pieced together over the last five years. I know #studyblr is a lie.
And yet. When I’m staring at my blank document and willing words to appear while my deadline ticks closer, immobile with fear that someone I love will get sick or that I will never hug my friends again or that I really was wrong about the whole Christianity thing and I am bound for a deluxe suite in hell, I take to Tumblr, and I pretend that my carefully-penned to-do list and my homemade iced coffee can get me through this. And, oddly enough, sometimes it does.
Mother Jones illustration; Ted S. Warren/AP; Getty
John still remembers the panic that gripped him when he first learned about the coronavirus. Detained at the Otay Mesa immigrant detention center in San Diego—with no access to masks or gloves and unable to practice social distancing—the asylum seeker from Cameroon knew he was vulnerable.
“Everyone was scared. We knew at any moment anything can happen,” said John, who is using a pseudonym to protect his identity. “If an officer came in with the disease, it was going to finish all of us.”
At the time, John had already been in detention for about five months. After fleeing violence back home, he had journeyed across South and Central America to seek asylum at the US border. He was taken into Border Patrol custody and sent to Otay Mesa, which quickly became the epicenter of the virus within the immigration prison system; to date, there have been 158 confirmed cases of COVID-19 at the facility, including the first person to die of the disease in ICE detention, a 57-year-old Salvadoran immigrant named Carlos Ernesto Escobar Mejia.
For John, the coronavirus only intensified his urgency to get out of detention as soon as possible. But first he’d have to post bond, the immigration detention equivalent to bail. Through a Catholic Charities legal services hotline, he had been connected to a pro bono lawyer, and eventually, in early March, an ICE deportation officer offered John the chance to be released on a $10,000 bond. If he couldn’t come up with the money, he’d be stuck inside, quarantined among an increasingly sick population at Otay Mesa.
“It was very stressful,” John said. His brother-in-law in Virginia was preparing to take him in, he said, but the $10,000 bond was too much for him to pay. “I had to cry out, I said, ‘Why me? I’ve been given this parole, but it’s this huge amount of money.’”
Like John, a majority of ICE detainees are eligible for release on bond while their cases move through the courts. Less than half of those who get bond hearings, however, are actually granted bond; as of March of this year, the national median granted bond was $8,000, but that number can easily go up to $40,000 in individual cases—an impossible sum for many immigrants to raise.
As the coronavirus has wreaked havoc in detention centers, local aid groups across the country have mobilized to help as many immigrants as possible post bond. For years, these community bond funds have stepped in with donations to help immigrants get out of detention. Like their counterparts in the criminal system that raise funds for pretrial bail, bond funds generally grow out of informal, local grassroots networks that raise bond money. But they’ve also come to form part of a nationwide fabric of volunteers, lawyers, and activists working to get people out of detention and support them after release.
Lee Wang, a former director of the New York Immigrant Freedom Fund, which has spent roughly $3 million since 2018 to release more than 400 people from New York and New Jersey detention centers, told me that before the pandemic hit they raised most of this money through foundation grants and public interest loans. Now, they rely almost entirely on grassroots fundraising, and they’re running out of money.
“Once COVID hit, it transformed everything overnight into an emergency campaign to free people for public health,” Wang said. “We’ve been able to keep paying bonds, but every week is a scramble and we will never have enough to free everyone who needs to get out.”
In the past few months, they’ve helped release nearly 60 people, double their normal rate. To meet with this increased demand, Wang has increasingly had to call on the National Bail Fund Network, 69 groups across the country that post bond and bail for people in the criminal and immigration detention systems. Normally, each fund raises and spends money within a local region, but they’ve had to do more cross-country coordination as individual funds scramble to get people out.
Even with continued fundraising and pooling different funds, the NBFN isn’t able to meet all the requests. “We’re zeroing out over and over again,” said Pilar Weiss, the network’s director. “As money comes in, it gets spent out.”
A parallel informal network exists within detention centers like Otay Mesa, as detainees share the phone numbers of people who might be able to help with bonds. That’s how John connected with NBFN, and his case ended up on the desk of Ana María Rivera-Forastieri, co-director of the Connecticut Bail Fund. In early April, she contacted John’s family members, who were waiting to receive him in Virginia, to let them know the network had raised the money and was going to post his bond.
But John’s detention nightmare was far from over.
Rivera-Forastieri went to an Enforcement and Removal Operations bond office in Hartford, Connecticut, on April 8, prepared to post John’s bond, only to be told by the ERO officer that there was no bond order for him. “We knew that wasn’t true,” she told me. “It’s hard to get ahold of these bond orders, especially during this time.”
Working with John’s lawyer in California and his family in Virginia, Rivera-Forastieri gathered the necessary proof of the bond order when she returned to the ERO office two days later. This time, however, they told her that John would not be released because he was in “quarantine hold.”
John told me that two people in his unit began showing symptoms of COVID-19 around this time, so the rest of the men in the dorm were quarantined together for 14 days in keeping with ICE’s policy of “cohorting” detainees exposed to the disease. (Cohorting goes against recommendations from the CDC and health experts, who have likened the policy to torture, saying that it can create a chain of infections, while also causing undue anxiety among detainees.)
ICE and CoreCivic, the private prison company that runs Otay Mesa, both confirmed this cohorting policy and maintain that efforts to contain the spread of COVID-19 are in accordance with federal guidelines.
“We asked when quarantine was over,” Rivera-Forastieri said. “But [the ERO officers] didn’t know anything. They said we ‘simply cannot post’ but didn’t give us any information.”
They found out from John that his quarantine would end on April 13. When Rivera-Forastieri went back to the ERO office to post bond, she again was turned away. This time, she was told, John had tested positive for COVID-19. He told me, however, that he was never sick, and while his temperature was taken regularly, he was never tested.
All the roadblocks and the dizzying relay of information between San Diego, Hartford, and Virginia began to take a toll. “It really penalized me,” John said. “They couldn’t pay, I had to stay here, and nothing was moving.”
“I felt a little paralyzed when all this was going down,” said Rivera-Forastieri, who doesn’t have many connections in San Diego—which meant John had to constantly update the various parties on his status from inside detention.
What’s worse is that all of these repeated trips to the ERO office wouldn’t have been necessary had ICE simply opened up its online “eBonds” system for making payments remotely to individuals and family members. But as of this month, it was still only open to for-profit bond companies. On April 1, the Congressional Hispanic Caucus wrote a letter to DHS requesting that this system be opened up to individuals and families, but so far no change has been made.
With every false start, Rivera-Forastieri had to organize—and then call off—a team of people who’d been put in place to help him get to his family after being released. These volunteers offer rides, shelter, and basic provisions for migrants as part of NBFN’s post-relief support. It’s another aspect of their work that has had to adapt to the new reality created by coronavirus, said Elizabeth Nguyen, who coordinates these efforts nationwide.
The danger of the pandemic has only served to highlight the urgent need to fix a system that is both riddled with red tape and is also, according to advocates, wildly arbitrary. That’s the latest argument the New York Civil Liberties Union is making in its lawsuit against the Justice Department over what it sees as unconstitutional bond practices that place an extraordinary burden of proof on migrants and unfairly detain people without consideration of alternatives, like ankle monitoring or community supervision programs, that have been proven effective. The case focuses on two immigration judges in Buffalo and Batavia, New York, who have denied bond in 95 percent of their cases. “This whole pandemic just highlights how the public interest isn’t being served by detaining people unnecessarily,” said Megan Sallomi, one of the attorneys on the case.
After many starts and stops, John’s case came to a head on April 23, when Rivera-Forastieri finally was able to post bond (which, at the 11th hour, was reduced to $5,000) in Hartford. John was subsequently released from Otay Mesa—roughly a month after the bond was first granted. By the time he crossed the threshold of the prison, NBFN post-release support had a ride (and a mask and hand sanitizer) waiting for him, lodging booked at a nearby hotel, and a plane ticket to rejoin his family in Virginia.
I spoke to John again recently, after he had been out of detention for a month. He sounded much more at ease, and glad to be with his family.
For the moment, he’d found what he’d been seeking when he set out for the United States: a sense of safety. He still had a long way to go to getting sustainable protection, but this was a hard-won battle—one he was determined to overcome.
“Even those who were ready to give up their case, everyone was fighting his way to get out of detention,” he said. “We were going to fight our fight.”
Prisoners at a federal correctional institution.David Zalubowski/AP Photo
The US Bureau of Prisons announced this week the death of Gregory Phinton Glenn, making him the 64th person in the federal system to die from the coronavirus and one of a growing number to die from the virus while serving time on drug charges.
Glenn had been serving a 14-month sentence for a drug use charge, a violation of his probation, at the Terre Haute federal prison in Indiana when he was taken to the hospital after testing positive for COVID-19 and exhibiting symptoms. Last month, the 56-year-old wrote a letter to the judge in his case begging not to send him back to prison. He explained that he was homeless and requested that he be sent instead to a halfway house in Davenport, Iowa, where he had previously received treatment. This request was denied, and he was ordered to serve the 14-month sentence. Glenn died on Sunday, a little over a month after he arrived.
Gregory Glenn’s letter to Judge John Jarvey of the Southern District Court of Iowa. PACER
Glenn’s use of K2, a synthetic form of marijuana, was a minor violation of his probation after a previous conviction in 2009. But as US prisons have become a hotbed for coronavirus infections, it proved to be a death sentence. 460 people across jails and prisons nationwide have died of the coronavirus to date. 41 percent of the federal inmates who died were imprisoned on drug charges.
Since the pandemic took hold in the US in early March, public health experts, politicians, and inmates themselves have been calling for the reduction of sentences and release of inmates—especially vulnerable people and those with low-level offenses—to home confinement. So far, some 70,000 people have been released, but very few of them have been from federal prisons like the one where Glenn was held. In a memo from early April, US Attorney General Bill Barr directed the Federal Bureau of Prisons to identify inmates who could be safely released to house arrest. But in the nearly two months since, ProPublica found that only 1.8 percent of people in federal prisons had been released.
In his unheeded letter to the judge asking for an alternative to prison, Glenn wrote: “I am asking you to give me another chance. The halfway house has tools that will help me get started in rebuilding my life.”
“You really think I would be promoting something that’s going to be giving vaccines to my people?” Trayon White, a city council member in Washington, DC, wrote in a comment on his Instagram post about the city’s initiative to hire contact tracers, officials who will locate the contacts of people in the city who test positive for COVID-19. The Black Democrat, who represents the city’s Ward 8, which has the highest number of COVID-19 deaths in the city, was responding to a commenter who was urging Black people not to get vaccinated.
White has come under fire for controversial statements—like the time he claimed that Jewish people controlled the weather—but he is beloved in the ward and seen as a fighter for a section of the city plagued by poverty, neglect, and rapid gentrification. Washington City Paper requested comment on the Instagram post, but the council member did not respond to explain what he meant. But for many Black people, he didn’t need to: His words reflected their unease surrounding medical racism and the mistreatment of Black people at the hands of doctors.
This is the side of the anti-vaxx movement rarely seen but in many ways much more mainstream in the Black and Brown communities. “We know that because of the history of segregation, discrimination, and racism there are reasons [Black] people don’t trust the government,” Sandra Quinn a public health professor at University of Maryland, explains. “The government doesn’t always have their best interest at heart.”
The anti-vaxx movement, as it’s become known, is comprised of a loose coalition of people in the United States and around the world who falsely believe that vaccines cause greater physical harm than any disease the vaccine purports to combat. They have already indicated their refusal to receive a vaccine for the novel disease should it become available.
These generally wealthier, whiter, suburban mothers are often more concerned with some idealistic notion of “choice” and “freedom” than with the findings of public health experts. They congregate on social media sites, sharing misinformation about vaccines causing autism in children, or the body’s capacity to heal itself. Vaccines can and do have side effects, and there have been batches of vaccines that have caused health issues in the past, but public health officials largely agree that overall they are safe and save lives. In recent years, an increasing number of measles outbreaks have begun to pop up around the country, as parents resist vaccinating their children for the contagious disease, which hasn’t been eradicated but was thought to be eliminated because of widespread, mandatory vaccination programs.
“Frankly, these Caucasian, suburban, educated parents believe they can Google the word vaccine and get as much information as anybody,” Paul Offit, the director of the Vaccine Education Center at Children’s Hospital of Philadelphia told the Philadelphia Inquirer.
But COVID-19 has highlighted the presence of another subgroup within the anti-vaccine movement: Black people, whose reasons for suspicion concerning vaccinations are rooted in a complicated mix of mistrusting the federal government, the shadow of having been experimented on before, and data that shows medical racism is endemic. Black people suffering from COVID-19 have frequently been turned away at hospitals, protests to “re-open” the economy surged after more news outlets started reporting on the disproportionate harm the virus was doing to Black people, and they frequently lack access to good health care due to structural inequality.
Some on the fringes have already announced their plans. Right-wing commentators like Candace Owens and YouTube stars turned conservative darlings Diamond & Silk have already announced that when the vaccine for COVID-19 becomes available, they will refuse to get it. Allegedly, the two hosts lost their show on Fox News’ streaming platform after Diamond and Silk specifically said they were rejecting any vaccine backed by Bill Gates—who has poured $300 million into the fight against COVID-19—because they falsely claimed the billionaire philanthropist pushed for population control.
It’s unclear why Owens said she would refuse a COVID-19 vaccine, but she has tweeted in the past about her own Bill Gates’ conspiracy theories and once claimed that she had a bad reaction to the HPV vaccine. She argued that this vaccine, which protects women against some cancers caused by sexually transmitted diseases, shouldn’t be mandatory because HPV is not contagious. To be clear: HPV is contagious.
This is your daily reminder that under no circumstances will I be getting any #coronavirus vaccine that becomes available.
The novel coronavirus has caused approximately 100,000 deaths across the United States and infected at least 1.7 million people. The disease caused states to close non-essential businesses leading to widespread job losses and economic calamity. Absent a miracle, scientists and health officials are warning that the virus will continue to spread in some capacity until an effective vaccine can be deployed around the globe. People of color have been disproportionately infected with and killed by this virus. According to data compiled and analyzed by my colleagues, Edwin Rios and Sinduja Rangarajan, in 20 of 28 states and the District of Columbia, Black people comprise a larger share of infections than their proportion of the general population.
As my colleague Jamilah King reported, it’s important that healthcare providers reckon with the legacy of racism that has left Black people skeptical of the medical community:
In response, health practitioners, particularly those who understand institutional and systemic racism to be a pre-existing condition for COVID-19, are now scrambling to fast track messaging to Black patients that doesn’t outright dismiss their concerns. I recently spoke with several doctors from across the spectrum of health care providers waging war against COVID-19 in New York City and in Georgia, where the novel coronavirus is disproportionately killing Black and Brown residents. While each suggests that it’s still too early in the pandemic to develop a complete set of hard and fast rules, or to tout specific successes, they largely agree that it’s absolutely crucial for medical personnel to acknowledge this history of racism when treating Black patients, affirming the reasons for their distrust, and then informing them with the best information available to date.
In a study Quinn did with her colleague Amelia Jamison, another public health expert at University of Maryland, and several others, one of the fault lines in the racial differences about vaccine skepticism can be foundin confidence in the government. When they studied trust in different institutions including drug companies, government institutions, and healthcare providers they found stark racial differences. “Nobody trusts the pharmaceutical companies,” Jamison explains. “But white people were generally more trusting of the government.”
In a May AP-NORC poll, 49 percent of people in the United States said they would take a COVID-19 vaccine. Thirty-one percent said they were unsure, while 20 percent said they would not take the vaccine. When broken down by race, the difference is dramatic: Fifty-six percent of whites were willing to take the vaccine but only 37 percent of Latinos and 25 percent of Blacks would do the same.
Despite the immediate public health emergency, the hesitance to take the COVID-19 vaccine may not be surprising. Along with anti-vaxxers who believe in pseudoscience, there are also legitimate concerns about the safety of a vaccine that is produced quickly. “The ongoing illness, death, and calls to socially distance will not alone change the minds of people who distrust vaccines,” Jennifer Reich, a professor of sociology at University of Colorado Denver said in a blog post. “The longer answer is more concerning: a new coronavirus vaccine and the ways government licenses, distributes, and communicates about it risk weakening support for all vaccines.”
One of the most frequent points of reference in explaining the deep and often well-founded suspicion of the medical establishment in the Black community is the 1932 Tuskegee experiment, 40-year clinical study to follow untreated syphilis in Black men. The study began in 1932 in Alabama, with 600 men—399 of them had syphilis while 201 did not. They were told they were being treated for “bad blood,” a colloquial term that encompassed a range of ailments, and were guaranteed to receive free medical treatment. In reality, the experiment’s true purpose was to study the progression of untreated syphilis. In 1972, the Associated Press published a story revealing the lack of treatment, the lack of consent, and the suffering that this community experienced from this study. After a Congressional hearing and a class action lawsuit, the men and their families were awarded millions of dollars in a settlement. But the stain remained, damaging the relationship between the African American community and health care providers. That distrust would play out during other public health crises for years to come.
While the researching the public health response to HIV/AIDS during the late 1980s, Quinn says the Black community was worried that HIV was a manmade virus created for the purposes of genocide. Some people believed it was created by the Central Intelligence Agency to kill Black people. Even though those conspiracy theories about HIV/AIDS have less currency today, when the disease first emerged, rumors about the origin were widespread.
In 2001, postal workers at the Brentwood Post Office and US Senate staffers in Washington, DC were exposed to anthrax after a terrorist mailed the harmful substance to US Senators. The vast majority of the postal workers were Black, while the Senate staffers were predominantly white. Following their diagnoses, both groups of employees deemed at higher risk were given antibiotics for 60 days. At the end of the 60 days, doctors recommended extending the antibiotic usage for another 40 days or receive a vaccine. Thirty-eight percent of the Senate workers and only 2 percent of the Brentwood workers chose the vaccine. Four years later, the American Journal of Public Health conducted a focus group of those same employees. Many of the Brentwood group were worried they were being used as guinea pigs and didn’t necessarily trust the vaccine because it was “experimental.”
The 2020 pandemic is unmatched in severity or scope, but the emerging conspiracy theories that have taken hold in the Black community feel familiar. Several have been making the rounds on social media, including that the virus is caused by 5G cell towers, and the vaccine (which has yet to be developed) will inject a tracking device inside of you. “The fears are always there, but they’re often raised from within the community,” Quinn says. “Now, they’re seized upon in social media and used to sow distrust and doubts about the vaccine.” It doesn’t help that the president has not disavowed the message from vaccine skeptics. After Diamond & Silk lost their show for promoting conspiracy theories around the virus and potential vaccines, the president tweeted praise for them.
Earlier this month, Trump announced Operation Warp Speed, a project to develop a vaccine at record speed in order to accelerate reopening businesses, schools, and returning to a normal life. According to polling data, the majority of the American public disapproves of the job the federal government is doing, making it a challenge to convince skeptics that a vaccine produced at record speed would be totally safe. In countries thought to have done a better job handling the pandemic, like South Korea and New Zealand, trust in the top level government officials is considered to have played a key role in containing the severity of the spread. In order to implement an effective national testing, contact tracing, and isolation strategy, Americans would have to put their trust in a government that has not inspired much of it. “The problem is that all the major scenarios for reopening the US economy are premised on trust,” Foreign Policyreported in April. “Will Americans really trust an entity—whether government, business, or nonprofit organizations—that compiles and tracks such personal data?”
Problems of trust in government aren’t unique to Trump. In 2009, the swine flu vaccine was considered an emergency vaccine because it had been quickly produced. Quinn studied the willingness to take an “emergency” vaccine among all the racial groups. Black people were more likely than any others to be skeptical of it.
Whatever the troubling history, it’s critical that the Black community take the vaccine when it is finally available. Not only are they more susceptible to the virus because of long-standing structural racism that has left them with a disproportionate share of underlying health conditions, they are also more likely to be employed in jobs that require constant contact with other people like transit workers, delivery drivers, and mail carriers. “Who’s most at risk?” Quinn explains. “We definitely need African Americans to get it. It’ll be devastating if they don’t.”
Can you pitch in a few bucks to help fund Mother Jones' investigative journalism? We're a nonprofit (so it's tax-deductible), and reader support makes up about two-thirds of our budget.
We noticed you have an ad blocker on. Can you pitch in a few bucks to help fund Mother Jones' investigative journalism?
This is where you come in.
We’re a nonprofit newsroom, because the truth-telling investigations we do don’t happen under corporate ownership. We get to shine a bright light into the dark corners of power and report stories other media are afraid to touch.
The essential ingredient that makes this possible? Readers like you.
We’ve got a lot of hard, consequential work to do in the weeks and months ahead, and we can’t do it without reader support. Please stand up for independent media and make a donation today.
This is where you come in.
We’re a nonprofit newsroom, because the truth-telling investigations we do don’t happen under corporate ownership. We get to shine a bright light into the dark corners of power and report stories other media are afraid to touch.
The essential ingredient that makes this possible? Readers like you.
We’ve got a lot of hard, consequential work to do in the weeks and months ahead, and we can’t do it without reader support. Please stand up for independent media and make a donation today.