Suzanne Prevost, the dean of University of Alabama’s Capstone College of Nursing, sent out an email on Thursday that elicited shockwaves through the university’s faculty. In the email, which went out to the nursing school’s faculty, Dean Prevost explained that she is “acutely aware” of the challenges of getting back to work right now and that those challenges are “especially pertinent for those of you,” she wrote in bold, “with school aged children.” She then implored her staff to let her know in advance if they would not be able to work in the fall so that the college will “have time to hire a new faculty member to replace you.”
“We wish that we had unlimited abilities to flex schedules and ‘make it work’ for everyone,” she wrote, “but this is just not the case.”
Dean Prevost wrote that she “wish[es] this thing would ‘just go away”’ and ended on the somber acknowledgement that”our wishes are not our reality.” (The word “wish” appeared four times in the email, suggesting that the resources Dean Prevost had at her disposal were tantamount to a pile of pennies aimed into an available fountain.)
Faculty at the @uaccn received this email from their dean yesterday directing instructors with children to consider quitting their jobs so that @UofAlabama can hire replacements. pic.twitter.com/d0JZ2sp6hx
As the Twitter thread on @SafeReturnUA‘s account pointed out, every University of Alabama faculty member has a right to twelve weeks of emergency Family and Medical Leave (FMLA) per federal law, which could cover paid leave should children have to remain home because of the coronavirus (most Alabama schools are planning to reopen in the fall). Her email also omitted information about how the University of Alabama has expanded FMLA following Congress’ passage of the Families First Coronavirus Response Act (FFCRA). The expansion provides more paid family leave benefits and emergency paid sick leave benefits, which faculty with children might find especially useful.
But many faculty at the College of Nursing are on contracts without long-term job security, making them more vulnerable to losing their jobs and the benefits that come with them. Identifying themselves as less available to work in the fall could jeopardize their chances for future employment at the University of Alabama, as made clear in the email. Despite repeated assurances from the University of Alabama’s administration that budget constrictions will not affect employees, four instructors in the English Language Institute recently did not have their contracts renewed. Since they were on contract, this technically does not count as a lay off or furlough.
Dr. Jack Carey, an instructor at the University of Alabama’s Department of American Studies, who is involved with the United Campus Workers of Alabama and the Safe Return UA initiative, said that the email is indicative of a broader issue at the University of Alabama, which is planning to reinstate in-person classes in the fall.
“It taps into this general pattern where you have a lack of transparency, no clear communication about what’s available to people, and the university putting the burden on the workers to deal with its plans to have face-to-face instruction,” he said. “I don’t feel like it’s clear to staff, even if they become aware of these opportunities for support, how to access them.”
Following the backlash to the email, which was reposted on Twitter and Facebook by United Campus Workers Alabama, Dean Prevost issued a statement on Friday clarifying that she “did not mean to suggest that any of you should resign from your faculty positions or that you will be terminated if you are unable to return to work.” The statement also linked to the paid family leave available to staff.
Aside from the confused messaging, why were only faculty members of the nursing school recipients of such a missive? Could it have something to do with their gender? According to the last census, nursing is a profession dominated by women—90% of the faculty at the University of Alabama’s College of Nursing use she/her pronouns on their website, reflecting the national trend.
I have to wonder whether the same email would have ever gone out to faculty at the College of Engineering.
When I contacted the University of Alabama for comment, they said that “the University has been clear about its support and understanding of the challenges facing faculty, staff and students during these difficult times” and linked me to Dean Prevost’s new statement. But that won’t erase the initial impression of the email, which was shocking even to faculty like Carey, who has worked in academia for many years and understands the how precarious the job market is.
“I was blown away by the email,” Carey said. “I’ve never seen anything like that.”
Schools across the country are set to open in mere weeks—some have announced exclusive virtual learning for the first months, others have promised to reopen with safety measures in place. But parents and staff continue to grapple with the confusion over what is safe and what isn’t while coronavirus cases skyrocket around the country. Are children of certain ages unlikely to catch the virus? Could they still be vectors? Are there ways for them to be together and still be safe? On Friday, the Centers for Disease Control published a case study with more bad news about kids and COVID-19, concluding that they “might play an important role in transmission.”
The study focused on an overnight camp in Georgia where, in June, 597 campers ranging in age from 6 to 19 and staff had gathered. The camp had some protocols such as requiring a test 12 days before arriving, having staff wear masks, and placing campers into smaller pods. But there were many ways the camp fell short of what public health officials have recommended: Campers were not required to wear masks, they shared cabins of up to 15 kids, and participated in a number of indoor gatherings. First, on June 23, a teenage staff member developed symptoms, and left. The next day, the camp began sending campers home and closed down on June 27.
Researchers found that the camp became linked to at least 260 infections among campers and staff. Children of all ages were susceptible to infection: 51 percent of the positive tests were for children who were from 6 to 10 years old, and 44 percent were 11 to 17. Of 136 cases with information about symptoms, 26 percent reported they had none.
The authors write:
These findings demonstrate that SARS-CoV-2 spread efficiently in a youth-centric overnight setting, resulting in high attack rates among persons in all age groups, despite efforts by camp officials to implement most recommended strategies to prevent transmission. Asymptomatic infection was common and potentially contributed to undetected transmission, as has been previously reported. This investigation adds to the body of evidence demonstrating that children of all ages are susceptible to SARS-CoV-2 infection and, contrary to early reports, might play an important role in transmission.
There are plenty of limitations to a case study, including that it’s possible kids became infected outside of camp, and no one can know with any certainty whether kids actually physically distanced or not. But the “attack rate,” or the number of positives, are also very likely an underestimate because of missed cases outside of the 344 tested. The camp became one of the largest super-spreader events in Georgia, where there are now 182,000 confirmed cases, more than 3,670 deaths, and 4,000 new cases added in a single day this week.
There’s still much we don’t understand about the role kids play in transmission and just how big an impact opening schools this fall will have on the still growing number of cases around the country. The political response hasn’t helped either, with Republicans like Georgia Governor Republican Brian Kemp banning cities and counties from issuing mask mandates. Parents have been left to face an impossible decision over with whether they should send their kids back to schools while science-denying politicians have given up on their responsibility to contain the pandemic. This latest study suggests that the consequences of reopening schools without stricter measures this fall may seed even worse outbreaks.
For a deeper dive into the confusing science over sending kids back to schools, read my colleague Jackie Flynn Mogensen.
A child wears a protective face mask in Kips Bay in New York as the city enters Phase 4 of re-opening following restrictions imposed to slow the spread of coronavirus Noam Galai/Getty
Over the past several months, it’s become abundantly clear that Black and Brown people in this country are at a much higher risk of contracting the coronavirus and dying from COVID-19 than their white counterparts. As my colleagues Edwin Rios and Sinduja Rangarajan have reported in detail, this is because “racism is a preexisting condition”; people of color are more likely to work essential jobs, to be uninsured, and to see higher rates of conditions like asthma and cancer due to disproportionate exposure to environmental hazards like highways and toxic dumping areas near their homes.
Now we have preliminary yet startling new data that reveals similar disparities in children, specifically in the case of MIS-C, a rare inflammatory illness linked to COVID-19.
The first reports of MIS-C, or Multisystem Inflammatory Syndrome in Children, were something of a mystery: In May, doctors in New York reported seeing otherwise healthy children enter the hospital with symptoms like fever, rash, vomiting, and diarrhea. They noted the condition was similar to Kawasaki disease, a decades-old condition that also afflicts children, but in this case, there was a clear coronavirus link: Most of the children tested positive for SARS-CoV-2 or had been infected before.
Shortly after these initial reports came in, the Centers for Disease Control and Prevention began tracking cases of MIS-C across the country. Government researchers have found that the condition is still relatively rare—only a few hundred cases have been reported nationwide—but there appears to be a deep disparity in who is ultimately stricken by the illness: Out of the 342 cases of MIS-C reported to the CDC, according to the CDC-defined categories of race, about 70 percent of cases have been in Hispanic or Latino and non-Hispanic Black children. Only 15 percent of cases have been in non-Hispanic white children. These are extreme differences: Consider that the US child population is reportedly about 50 percent non-Hispanic white, 25 percent Hispanic, and just over 13 percent non-Hispanic Black.
It’s still unknown exactly why Black and Latinx children are disproportionately burdened with this disease, but it’s clear that those populations, including children, are seeing high rates of COVID-19 infection to start with. Where data on race is available, again using the CDC-defined terms, Hispanic or Latino children make up about 47 percent of COVID-19 cases between the ages of 5 and 17; non-Hispanic Black children make up about 17 percent of cases; and non-Hispanic white children make up about 27 percent of cases. (The CDC collects data on children younger than 5 in separate reports, but the same trend holds true.)
High rates of COVID-19 infection may partially explain why so many Black and Latinx children are later developing MIS-C, though researchers say that is far from certain. “If you look at the population as a whole, exposure to the virus—there is a lot of Black and Hispanic overrepresentation,” says Dr. Adrienne Randolph, an author ofa recent CDC-funded nationwide study aimed at better understanding how children are impacted by MIS-C.“It’s hard to know where people are exposed to the virus, but if they’re getting exposed in their home or home community, then that may be why children are getting exposed more and then getting MIS-C more. That’s the assumption. But that has not been proven.”
The CDC echoed this conclusion in an email to Mother Jones, saying, “We can speculate that the disproportionate impact of MIS-C on Black and Hispanic/Latino children and youth is reflective of the disparate exposure to and risk of serious illness from COVID-19 that we’re seeing among Black and Hispanic/Latino adults; however, further research is needed as what we learn about MIS-C continues to evolve.”
Aside from the high rates of exposure to this coronavirus, it’s also possible there’s something in the kids’ environments that make them more vulnerable to MIS-C. For example, Randolph says, Black and Latinx communities see higher rates of asthma due to disproportionate exposure to environmental “triggers” like air pollution.
Randolph, who is also a senior associate in the division of critical care at Boston Children’s Hospital and a professor of anesthesia at Harvard Medical School, and others are currently working to fill in these gaps in our understanding. She is assistingthe CDC in designing a study to monitor children who test positive for SARS-CoV-2, to see who does and doesn’t develop MIS-C later on, while tracking factors like race and ethnicity. This won’t fully answer the question of why Black and Latinx children are getting sick at higher rates, she says, but may provide a “little bit of a hint.” The next step, she says, would be to conduct a study in which families are interviewed by researchers to determine what risk factors they may have faced before getting sick. The CDC is currently designing such a study, she says.
As schools move to reopen, she says, researchers will need to be ready to track who is getting infected, where they’re getting infected, and if complications like MIS-C are arising. “It’s important to design studies going forward that would capture the right data to answer those questions,” Randolph says, though she cautions that robust, forward-looking studies can be difficult to carry out.
“It’s a very concerning problem and it really needs to be addressed,” she says about MIS-C. “And we’re trying to get more answers as best we can, but it’s not gonna be an easy question to answer.”
This post has been updated to include the CDC’s response.
Last week, a small rural county in south Texas went from the poster child for good pandemic response to the entire country’s worst nightmare.In a widely-covered press conference, Starr County Health Authority Jose Vasquez announced that, like many hospitals in Texas’ Rio Grande Valley region, the local hospital had reached capacity for COVID-19 patients and they had adopted a plan to start triaging the sickest patients. While that meant allocating the dwindling ICU beds to patients the most likely to survive treatment, some media outletsacross the country sounded the alarm on the soon-to-be-formed “death panel” that would decide which patients would be saved at Starr County Memorial Hospital, and which would be “sent home to die.”
This week, however, things are actually … looking up? (Hold onto that, you won’t get it much in 2020.)In the wake of the media frenzy, Texas Gov. Greg Abbott sent Navy teams to help out hospitals in the Valley, including Starr County’s tiny 29-bed COVID-19 unit. According to Thalia Munoz, the hospital’s CEO and administrator, a hospital in San Antonio, nearly 250 miles away, has allowed them to start transferring patients to their facility. The “death panel” was called off.
“I don’t want to say everything is OK,” Munoz told Mother Jones on Wednesday, “but we’re starting to see the light at the end of the tunnel.”
Still, while the state’s recent response to the dire situation along the Texas border is certainly welcome, some say the situation never should have gotten this dire to begin with. They argue Abbott’s own inaction early in the pandemic, as well as his efforts to reopen the state back in early May—at the expense of local control—was part of what put these communities in this situation in the first place.
Early in the pandemic, numerous advocacy groups and local media outlets warned that places like Starr County were particularly vulnerable to the coronavirus. The Rio Grande Valley’s residents are more than 90 percent Latinx and have one of highest poverty rates in the state; nearly half are uninsured and chronic health conditions abound—the rate of diabetes in the Valley is triple that of the national average, for example. In nearby Hidalgo County, the coronavirus fatality rate is more than twice that of the state’s overall average.
“My concern is not only that it is circulating without our knowledge, but we also have a population at high risk for severe disease,” one epidemiologist told the Texas Tribune in early April. “I don’t think it will take very long at all to overwhelm the facilities at our hospitals.”
A few weeks later, I had an eerily prescient conversation with medical ethicist Nancy Berlinger about triage in the hospitals in New York City, then the country’s most severe coronavirus hot spot. “The tremendous effort on the part of governors and hospitals to get ventilators and beds into places where they were needed staved off the need for triage, but that doesn’t mean it won’t happen,” she told me. “Remember, in some parts of the country, where you’re just beginning to see outbreaks, you might have much smaller hospitals. We’re gonna have to keep an eye on some of these outbreaks that we’re seeing in very rural states because the local hospital might be very small, or it might be a quite a long way away from where the population is. So no, nothing is over.”
At Starr County Memorial Hospital, the staff—sans triage committee—is working hard to care for their community. But some damage has already been done. One nurse told me last week’s discussion of “death panels” was a misrepresentation of her on-the-ground reality and disheartening for both frontline workers and residents who, for a myriad of reasons, are already hesitant to seek medical care. She said between the at-risk patient population they worked with and the state’s rush to reopen, medical workers were just doing their best in a worst-case scenario.
Bryn Esplin, a medical ethics expert and professor at the University of North Texas Health Science Center, told me blaming doctors in chronically underfunded and underserved areas misses the mark. “No one wants to decide who lives and who dies,” Esplin said. “It’s an excruciating decision that leads to burn out and moral distress. But these heart-wrenching decisions [almost had] to be made all because of social priorities and structural racism.”
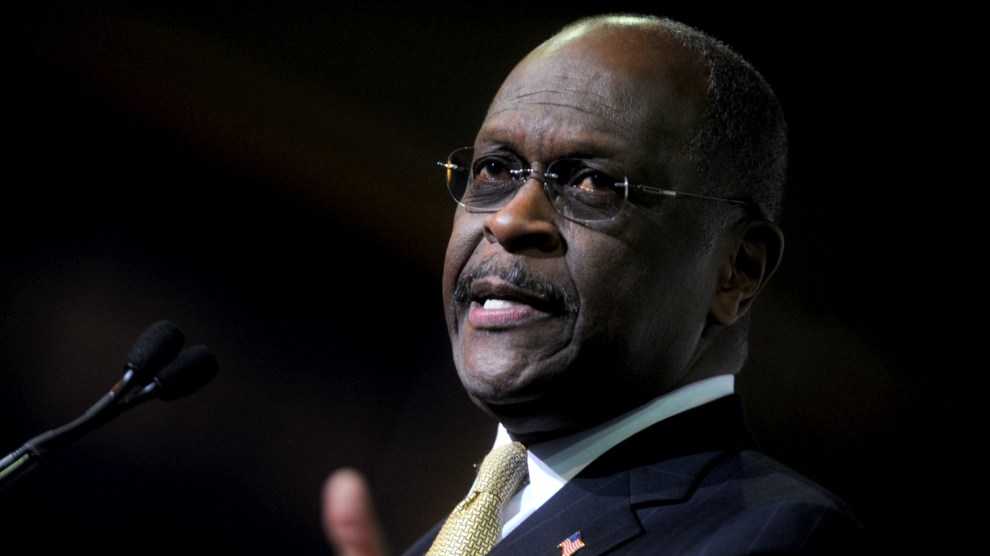
Herman Cain—the businessman, Tea Party conservative, and 2012 Republican presidential candidate—has died of complications from COVID-19 at the age of 74.
Cain had appeared without a mask at President Trump’s June 20 rally in Tulsa, though it is not known where and when he contracted the coronavirus. He tested positive for the virus on June 29 and had been hospitalized since July 1, according to a message posted on his Twitter account.
Cain was a successful businessman who helped boost sales at Burger King and Godfather’s Pizza in the 1980s. His other roles included chairman of the Federal Reserve Bank of Kansas City and economic adviser for Bob Dole’s 1996 presidential campaign.
Cain gained prominence in the race for the 2012 GOP nomination with his proposed “9–9–9 Plan,” which suggested replacing the existing tax structure with a 9 percent personal income tax, 9 percent federal sales tax, and 9 percent corporate tax. He withdrew from the race in December 2011 after several women accused him of sexual misconduct. (He denied the allegations.)
Cain was a staunch supporter of President Trump and co-chaired Black Voices for Trump. In 2019, Trump attempted to nominate him for a seat on the Federal Reserve Board, but Cain withdrew his name from the nomination pool amid resistance from Congress—and after learning that he would have to give up most of his business interests.
Philanthropist and ex–New York Mayor Michael Bloomberg reacts to a joke at his expense at a 2014 charity gala.AP Photo/John Minchillo
If you’re one of the 10 percent of Americans who works for a nonprofit, you’re biting your nails right now. A CNN commentator recently called COVID-19 an “extinction-level event for America’s nonprofits.” Philanthropy News Digest reports that 83 percent of nonprofits have seen a drop in revenue between March and June 2020. Seventy-one percent say they can’t provide the same services they once did. The number of nonprofit staff dropped by almost half amid a torrent of layoffs and pay cuts. And philanthropic grants are down by a third. No wonder, right? Who has loose change to give away at a time like this?
Billionaires do.
The biggest philanthropists, the ultra-rich, are doing great. Between March 18 and June 5, American billionaires added more than half a trillion dollars to their collective net worth. Thanks to growing inequality, small-dollar donations to charity are being replaced by upper-class philanthropy. But upper-class philanthropy is a lot less likely to make its way to people in need.
Those are the conclusions of a new report from the Institute for Policy Studies, a DC-based progressive think tank that backs an overhaul of charity laws. The number of donors is falling—by 12 percent from 2009 to 2019, the report finds, likely because stagnant wages and growing inequality have made it difficult for many small donors to keep giving. In 1989, 81 cents of every dollar that went to charity came from an individual. In 2019, that figure was 69 percent. On paper, the richest Americans have made up for a drop in middle- and working-class donations. In practice, their donations are more likely to gather dust—and tax deductions.
Where small donors have traditionally given to working nonprofits, wealthy donors prefer donor-advised funds and foundations. (Donor-advised funds, increasingly popular with investors, let you donate, collect a tax deduction for the full value, and decide what to do with the money later. The Chronicle of Philanthropy calls them a “personal charitable savings account.”) That money—even when it comes in large amounts, or “mega-gifts”—doesn’t always trickle down to the grassroots organizations it’s supposed to help. In fact, most charitable foundations don’t have to spend more than 5 percent of their funds per year. Whether or not they give to working nonprofits, they’re still able to shield donors from the IRS by allowing billionaires to write off their contributions as tax deductions.
Video
Related: Mike Bloomberg Is Way Richer Than People Realize
The UC Berkeley economist Gabriel Zucman has called mega-gifts the equivalent of a “tiny, tiny wealth tax.” The top 20 US billionaires after Bill Gates and Warren Buffet, Zucman writes, donated about 0.3 percent of their wealth in 2018. The catch: It’s barely more than the taxes they’d owe on half their wealth, even under our billionaire-friendly tax code. More than 200 ultra-rich donors have picked up great press for the Giving Pledge, a Gates/Buffet-led initiative to give away most of their assets. But as IPS points out, if the US signers gave away half of their net worth—$485 billion, including to their own foundations—they’d be shorting Americans $360 billion in taxes, given that they’re able to write off so much of their contributions. Unfortunately, donations to museums, universities, and even public health programs can’t replace the essential function of taxes: to float social goods like working transit, housing subsidies, unemployment insurance, and public education.
If you see an uncanny echo of dark money in politics, you’re not wrong. When small, individual donors get squeezed out, the report says, charities have to start responding to what a few big donors want. IPS calls it “mission distortion.” Despite bringing in massive tax breaks, much of the almost $16 billion donated by the top 50 philanthropists in 2019 “may not actually get into the hands of active public charities for years—or ever, potentially, in the case of donor-advised funds.” Even when mega-gifts do go to active working charities, the report notes, “they tend to be directed toward larger organizations, and towards causes that the wealthy prefer.” The most popular targets for those mega-gifts were the donors’ own private foundations.
Many private foundations are deeply entwined with offshore trusts and tax havens: Illinois governor and billionaire Hyatt heir J.B. Pritzker squirreled significant shares of his estimated $3.5 billion net worth into a tangle of Carribean trusts and holding companies, all of which funnel cash into his private foundation. (Other members of the Pritzker family have donated to Mother Jones.) America’s richest family, the Waltons, runs a foundation that sits on nearly $5 billion in assets. And “99 percent of the Foundation’s contributions since 2008,” one Forbes contributor reports, were made through trusts “specifically designed to help ultra-wealthy families avoid estate and gift taxes.”
And some foundations could use way more oversight. The Trump Foundation dissolved in 2018 after a complaint from New York’s attorney general accused it of a “shocking pattern of illegality,” including collusion with the Trump campaign, calling it “little more than a checkbook” for Trump’s “business and political interests.”The opioid–rich Sackler family—some of whom own Purdue Pharma, which has come under increasing scrutiny for aggressively hawking OxyContin—has lent its name to the Mortimer and Theresa Sackler Foundation, the Sackler Trust, the Raymond and Beverly Sackler Foundation, La Fondation Sackler, and the Arthur M. Sackler Foundation—among others.
The Sackler and Walton names, among others, are splashed across institutions, from art galleries to hospitals and universities (although many museums, along with Tufts University, have now stripped references to the Sacklers from their buildings). That doesn’t always bode well for small charities. From the report:
Top-heavy philanthropy favors bigger charities that already have sophisticated major donor programs, the capacity to manage and implement gifts of enormous size, as well as the infrastructure to accommodate gifts of appreciated stock and high-value noncash assets. This may put smaller, more independent, and potentially more innovative and nimble organizations at a disadvantage.
In other words, high-dollar philanthropy more often looks like equity billionaire David Booth’s $300 million gift to the already-very-rich University of Chicago’s business school—now the Booth School of Business—rather than a big check for scrappy youth organizations, prison abolitionists or hyper-local environmental justice groups like those backed by Resist, a nonprofit that makes modest grants to grassroots organizers. From 2017 to 2018, the Chronicle of Philanthropyfound that giving to the 100 biggest charities grew 11 percent, even as giving fell overall. Nonprofit Quarterlysays we live in an age of “philanthropic plutocracy.” And since 1985, according to Berkeley’s Zucman, foundation wealth has grown by more than half as a share of household income. Foundations now hold more than $1 trillion in assets, he writes.
Charity rules, drawn up in 1917 to benefit the Gilded Age rich, worked best in the postwar years, when millions more Americans had cash to throw around—which they did, consistently, at a rate of around 2 percent of their incomes. But when those incomes stagnated, charities leaned more and more on Walmart heirs parking billions in family foundations and dodging capital gains while they vote with their wallets. Are we really better off for that?
Rep. Louie Gohmert, a Texas Republican who for months has steadfastly not worn a mask nor maintained social distancing in the halls of Congress, has tested positive for COVID-19, according to multiplesources. Gohmert was scheduled to fly with President Donald Trump to Midland, Texas on Wednesday to attend a fundraiser and tour an oil rig. According to CNN, Gohmert tested positive for COVID-19 during a pre-flight screening at the White House and is now not joining the president’s convoy to Texas.
Even among Republicans, Gohmert stands out as one of the few who refuses to wear a mask when not mandatory (House rules mandate that all members of Congress must wear a mask during in-person committee hearings). On Tuesday, Gohmert attended two House hearings, including the judiciary committee’s hearing with Attorney General William Barr. Prior to the hearing, Gohmert was captured on video walking with Barr, both men unmasked. Politicoreports that Barr will be tested for COVID-19 at some point Wednesday.
ACTUALLY… here is a video of AG Barr and Gohmert.
While Barr arrived with a mask, it was off when he walked into the hearing room, so both men were not wearing masks at this time. pic.twitter.com/xm6wuq6QvW
In June, Gohmert tried to explain why he doesn’t where a mask, giving CNN an answer that “defied the science and the recommendations of leading public health experts.” But he said that if he were to get coronavirus, “you’ll never see me without a mask.” After learning that he had tested positive for COVID-19, Gohmert told his staff the news in person. It’s unclear if he was wearing a mask.
In an email to Politico‘s Jake Sherman, an aide in Gohmert’s office said that the Texas congressman requires his all of his staff to work in his Washington, DC office so they “could be an example to American on how to open safely.” Gohmert also allegedly berated his staff for wearing masks.
Here’s a tip for boosting White House press conference viewership: Spend more time discussing alien DNA.
The topic arose during President Trump’s Tuesday afternoon coronavirus briefing after he doubled down on his belief that hydroxychloroquine is an effective treatment for COVID-19, despite a dearth of evidence supporting this claim. On Monday night, Trump retweeted a video in which a group of doctors touted the drug as a cure for the coronavirus. Twitter deemed the doctors’ claims so egregious that it deleted the tweet and penalized Donald Trump Jr., who’d also shared the post, for spreading misinformation.
Trump didn’t seem to see the problem with the video. “There was a group of doctors yesterday, a large group, that were put on the internet, and for some reason the internet wanted to take them down,” he said at his press briefing. “There was a young woman who was spectacular in her statements about [hydroxychloroquine], that she’s had tremendous success with it, and they took her voice.”
That young woman subscribes to some rather outré theories, among which is her belief that dream-sex with witches and demons causes gynecological problems. (The myth of the incubus dates to the third millennium BCE.)
“The woman that you said was a great doctor in that video that you retweeted last night said that masks don’t work and there is a cure for COVID-19, both of which health experts say is not true,” CNN’s Kaitlan Collins said. “She’s also made videos saying that doctors make medicine using DNA from aliens, and that they’re trying to create a vaccine to make you immune from becoming religious.”
“I can tell you this,” Trump replied. “She was on air, along with many other doctors, and they were big fans of hydroxychloroquine, and I thought she was very impressive, in the sense that from where she came—I don’t know which country she comes from—but she said that she’s had tremendous success with hundreds of different patients, and I thought her voice was an important voice, but I know nothing about her.”
To be fair, Trump most likely knows nothing about the doctor’s demon-sex theories, which were originally unearthed by the Daily Beast. But that certainly doesn’t make it any less hilarious to watch the president defend a doctor who seems to have gotten her training at the Boris Karloff School ofMedicine. Here’s the video:
Trump's new "important voice" is a woman who…checks notes…believes that dream sex with demons causes gynecological problems? pic.twitter.com/F78KaMkhaJ
Addressing the nation from the Bioprocess Innovation Center in North Carolina, President Trump on Monday painted an optimistic picture of the United States’ recovery from the coronavirus pandemic—while dismissing one of the only proven ways to mitigate the spread of the virus in the first place.
“I really do believe a lot of the governors should be opening up states that they’re not opening,” he said in response to a question about whether the US economy would see a V-shaped recovery. Despite a recent surge in cases in Texas, Republican Gov. Greg Abbott, whom Trump praised on Monday, has refused to shut down the state’s economy.
Trump also announced that the biotechnology company Moderna had entered phase 3 of vaccine development, meaning that the company’s COVID-19 vaccine is now being used in clinical trials. “We will achieve a victory over the virus by unleashing America’s scientific genius,” he said, flanked by screens bearing the words “Operation Warp Speed.”
If only there were another way.
Video
Related: Trump’s First 100 Days of Deadly Coronavirus Denial
Update, July 25, 4pm ET: Sinclair says it will “delay” the broadcast of America This Week featuring Judy Mikovits.
The discredited researcher behind “Plandemic”—a viral video that falsely suggests the coronavirus is “activated” by face masks, amid other bizarre claims—is set for a major revival this weekend. And you have the Sinclair Broadcast Group, which has drawn criticism for its ultra-conservative, pro-Trump programming, to thank.
On the show America This Week, which is distributed to hundreds of local news stations operated by Sinclair, host Eric Bolling interviewed Judy Mikovits, the virologist whose wild assertions about the coronavirus and infectious diseases expert Dr. Anthony Fauci are at the center of “Plandemic.” The interview, which was first reported on by liberal watchdog group Media Matters, included chyrons asking, “Was COVID-19 Created in a Lab?” and “Did Dr. Fauci Create Coronavirus?”
Sinclair is now airing straight-up coronavirus conspiracy theorists (of "Plandemic" notoriety) across the country. A point of discussion was whether Fauci created covid himself. Unspeakably irresponsible. More via @mmfa@zpleat here: https://t.co/eNUC2AyWMupic.twitter.com/cZSrkkQQ52
Mikovits gained notoriety in May for her starring role in “Plandemic,” a 26-minute video asserting several misleading or false theories about Fauci and the origin of the coronavirus. The video, which was viewed more than eight million times in one week despite being removed from most social media platforms, is supposedly excerpted from a forthcoming movie, which aims to “expose the scientific and political elite who run the scam that is our global health system.”
Originally a chronic fatigue syndrome researcher, Mikovits has become an icon of the coronavirus-skeptic community for her outlandish allegations, including that a possible virus vaccine will “kill millions.” She also has carried a long personal grudge against Fauci, who she holds responsible for her personal downfall. In November 2011, Mikovits was arrested and charged with stealing property from her previous employer, a nonprofit medical research center in Nevada. The charges were ultimately dropped, but in “Plandemic,” Mikovits described the case against her as a vast government conspiracy spearheaded by Fauci. “He directed the cover-up,” Mikovits says. “And, in fact, everybody else was paid off, and paid off big time.” But, as the University of Pennsylvania’s FactCheck.org reported, “at no point in the video does anyone explain what Fauci supposedly covered up.”
In the interview with Bolling, Mikovits said Fauci “manufactured” the coronavirus at a military base in Maryland and “shipped” it to Wuhan, China. She cited no evidence. Bolling did not push back, only acknowledging it was a “hefty” claim—though Bolling insisted to CNN, that was him challenging her. He also told the network he was completely unaware of her role in “Plandemic.”
Sinclair, originally founded in Baltimore, has become one of the largest local television providers in the country and well known for its pro-Trump programming. Before he was dropped last year, former Trump adviser Boris Epshteyn sparked controversy for saying during a political commentary segment for Sinclair that migrants were mounting an “attempted invasion” of the United States; Sinclair apologized for the remark and eventually moved Epshteyn into a different role within the company. All this is particularly problematic since, as CNN notes, public opinion research shows more Americans trust their local news than media more broadly.
The Supreme Court on Friday rejected a Nevada church’s attempt to circumvent state limits on attendees at religious services during the coronavirus pandemic. Chief Justice John Roberts joined the court’s four liberal members in ruling against the church, which had said it was unfair for houses of worship to be limited to 50 attendees, while casinos in the state could still operate at 50 percent occupancy.
Roberts’ deciding vote sent right-wing Twitter, and at least two US senators, into a frenzy.
“John Roberts has abandoned his oath,” Sen. Ted Cruz (R-Texas) tweeted early Saturday morning. “But, on the upside, maybe Nevada churches should set up craps tables? Then they could open?” Cruz’s post included a screenshot of Justice Neil Gorsuch’s one-paragraph dissenting opinion, which said, “In Nevada, it seems, it is better to be in entertainment than religion.”
Roberts, a George W. Bush appointee, is no one’s idea of a #Resistance hero, but he has repeatedly angered conservatives by siding with the court’s liberal minority in certain high-profile cases. In 2012, he famously saved the Affordable Care Act by declaring it a tax. Last month, he joined a 5-4 vote to protect abortion rights (at least for now). And he recently wrote the court’s opinion blocking President Donald Trump from immediately ending the Deferred Action for Childhood Arrivals program.
Sen. Tom Cotton (R-Ark.), who said after the abortion case that Roberts was “apparently more concerned with liberal opinion than with doing the right thing,” had more sharp words for the conservative jurist following the Nevada church decision:
John Roberts at his hearing: “If the Constitution says that the little guy should win, the little guy’s going to win in court before me.”
What happened to that judge?
He didn't mention his belief that casinos have more rights than churches. https://t.co/KjpyLbkIMo
On a more conservative court, Roberts has increasingly become the swing justice, making him an easy target for right-wing purists. Rep. Doug Collins (R-Ga.), who is in the midst of a tightSenate race in Georgia with Republican Sen. Kelly Loeffler, called the Nevada ruling “another horribly disappointing” Supreme Court decision. Mike Huckabee, the former Arkansas governor and prime candidate for weirdest tweeter of the decade, had perhaps the strongest condemnation of Roberts on Saturday:
Thanks @realDonaldTrump for appointing Gorsuch. Too bad Chief In-Justice John Roberts is so swamp-infected that he protects casinos & punishes places of worship. He needs to retire, but first he just needs to repent! https://t.co/ZFjyvxTRn6
— Gov. Mike Huckabee (@GovMikeHuckabee) July 25, 2020
Trump himself was relatively muted about the decision on Saturday morning, and didn’t call out Roberts by name—even though he has not been reluctant to criticize the justice directly in the past. In 2012, he sent off a flurry of not-so-nice tweets in the aftermath of the Obamacare ruling:
John Roberts arrived in Malta yesterday. Maybe we will get lucky and he will stay there.
Since taking office, Trump has railed against the “Obama judges” who declare his policies unconstitutional, sparking a rare rebuke from Roberts and—inevitably—more tough talk from Trump. The president has kept the court high in Republican voters’ minds as a key issue for 2020, tweeting after the recent DACA decision about these “horrible & politically charged decisions coming out of the Supreme Court,” adding that conservatives “need more Justices or we will lose our 2nd. Amendment & everything else.”
On Saturday, in response to the Nevada ruling, he had a much more succinct message: “Win in 2020!!!”
In a reversal of his previous plans, President Trump announced Thursday that the portions of the 2020 Republican National Convention scheduled to take place in Jacksonville, Florida will be cancelled.
The official business of the RNC—delegates’ nomination of a Republican presidential candidate—will still take place in person in Charlotte, North Carolina, the original convention site. When North Carolina Gov. Roy Cooper declared the three subsequent days of speeches and celebrations unsafe amid the coronavirus pandemic, ceremonies were relocated to Jacksonville. Now, they’re cancelled too.
I love the Great State of North Carolina, so much so that I insisted on having the Republican National Convention in Charlotte at the end of August. Unfortunately, Democrat Governor, @RoyCooperNC is still in Shutdown mood & unable to guarantee that by August we will be allowed…
Despite Trump’s previous insistence on holding a full in-person rally to celebrate his nomination, he painted the decision to cancel the event, which he announced at his third coronavirus briefing of the week, as his idea.
“I looked at my team and I said, ‘The timing for this event is not right, just not right, with what’s happened recently, the flare-up in Florida, to have a big convention,” he said. “It’s not the right time.'”
“They said, ‘Sir, we can make this work very easily,'” he continued, before launching into a tangent about the “senseless violence” he claims is plaguing American cities. “I said, ‘There’s nothing more important in our country than keeping our people safe, whether that’s from the China virus or the radical left mob that you see in Portland.'”
As the world grapples with the devastation of thecoronavirus, one thing is clear: The United States simply wasn’t prepared. Despite repeated warnings from infectious disease experts, we lacked essential beds, equipment, and medication; public health advice was confusing, and our leadership offered no clear direction while sidelining credible health professionals and institutions. Infectious disease experts agree that it’s only a matter of time before the next pandemic, and that could be even more deadly. So how do we fix what COVID has shown was broken? In this Mother Jones series, we’re asking experts from a wide range of disciplines one question: What are the most important steps we can take to make sure we’re better prepared next time?
Andy Slavitt knows the ins and outs of public health in America. After decades of leadership in health care companies, he served under President Obama as the acting administrator for the Centers for Medicare and Medicaid Services, where he was instrumental in implementing the Affordable Care Act. United States of Care, the nonprofit he helped build in the years since, aims to improve access to health care for all Americans.
Slavitt grasped the seriousness of the coronavirus back in February, when he urged the White House to ramp up preparations—and he wasn’t shy about criticizing what he saw as a woefully inadequate response. In March, he predicted the shortage of hospital beds and ventilators. Since then, he’s emerged as an authority on both the medical and political dimensions of COVID-19. His podcast, “In the Bubble,” tackles vaccine science, offers advice on confronting mask deniers, and offers solutions to the emerging hunger crisis as the economy falters. His prolific Twitter feed is required coronavirus reading—in voiceythreads, he contextualizes the torrent of overwhelming pandemic news. Earlier this week, he summed up what seems like his guiding principle in a single tweet: “Crises are shorter when governments are better.”
On the three biggest things we can do to prepare for the next pandemic: I gave a speech at School of Public Health at the University of Minnesota in December—little did I know how close we were coming to a pandemic—and I said that the biggest problem in public health is there is no effective public health lobby and no one had put together a case for $100 billion of investment in the country’s public health infrastructure. Here we are, $4 or $5 trillion later, and $100 billion seems like a dream.
We need to be able to do very quick tracing and testing and have that infrastructure up and ready to go. We also need the physical infrastructure, a cache of ready supplies, probably in regional hubs that are continually maintained. For this particular crisis, we know that looks like masks and shields. But depending upon how something spreads, it could be other things. And along with that, we need a domestic drug supply manufacturing capacity so we can control some of the critical medications and not have to rely on overseas trade. I’m quite sure we can get the literal things right. We probably will never run out of ventilators again. But it’s a little bit like responding to 9/11 by saying, “Okay, now we can’t bring water into the airport anymore.” Very literal, right? But that will miss the more substantive lesson.
The second category is health care resilience. We have a health care system where access is tied to employment, and when employment goes down—and it often does in crises like this—people lose access. Another example is the fee-for-service model in hospitals, which stop getting any money when people stopped using elective services. This can also be something we can anticipate in a pandemic. And that money instead is with insurance companies who are supposed to be middlemen. They’re not supposed to be sitting on the money for people. It should be in the community, investing in public health. So you have to change the way care providers are paid. And you have to separate people’s access to health care from whether they’re working.
The third thing is the psychological element to preparedness. We don’t think about public health events. Right now, you can’t go to a major corporation or a school district and say, “Who’s your expert or leader about the health of the population?” And that’s going to need to change at every level. Starting at the federal level, we probably need a cabinet-level position to respond to biological threats, the equivalent of what we did when we created the Department of Homeland Security. It could be done somewhere else. But I think you want somebody who has accountability to the president. We have a president who tore down the infrastructure, and we can’t ever let another president do that again. The safest way for Congress to do that is to create a cabinet responsibility.
But not just at the federal level. I think we need to do that at the state level and at the corporate and company level, at the municipality level. And what that will mean is lots more people having the opportunity within public health as a career. People could work for Google and be in their public health department. Or you could work in a municipality and think about the health issues there. That’s what it’s going to take to have more public health consciousness, rather than having to go back to where it was before the pandemic, which is something that can’t get funded, or continually gets its funding cut.
On Trump-proofing the public health system: You can’t Trump-proof anything. People who want to destroy things and act like little children and have temper tantrums—you shouldn’t elect people like that. Take the CDC: Basically, over time, Trump wanted to neutralize and antagonize the scientific community. He did the same thing at EPA. The lesson for the American public is that in electing a president, you’re electing the entire government.
But I think if you bake in a cabinet-level position with congressional oversight, you have better checks and balances at least. And then, of course, you have to have sufficient funding that goes to the states so you don’t have to have states that are begging and pleading for every dollar.
On the culpability of White House coronavirus response coordinator Dr. Deborah Birxin reopening too early: We can debate whether it was because she was politically trying to please Trump, or because she didn’t see and understand the data correctly. But ultimately she made the wrong call. And it’s not like, “Oh, well this is 20/20 hindsight, she made a mistake, which happens.” Everybody saw what she didn’t see. The lesson is not: it’s not about Birx, it’s about Trump. Because if you cherry-pick the advice you take and make it clear that you only want answers that suit you, then you will pigeonhole yourself. A good president—and I only have experience with one, President Obama—knows how to seek advice and counsel from all quarters to make sure every option is on the table. I’m pretty certain that if Trump had said, “I am open to whatever option you want to put on the table, including things that keep the government shut down,” she would have put different options on the table. I think he hedged her into, “I’m opening May 1, you need to show me how.” That’s not the right way to seek advice from your senior advisors. I don’t let her off the hook. She made a mistake. She should have done better. But it starts with the way Trump manages.
On schools: Next time, it will be great to have red-teamed all of these situations. Who can go to school safely if they don’t live with anyone immunocompromised? Do you have the kind of space you need? Can we get better at distance learning? And if so, what’s the age group where it’s effective and ineffective? If we’re able to know these things going in, then we can have a contingency plan, and it doesn’t have to be this kind of crisis. Right now, we don’t have backup plans, because in this country, we run real-time and efficient. There’s a broad lesson that applies to different elements in society around contingency planning. One of the fallacies of the idea that you starve the government until you need the government is that you end up spending ten times as much money and you spend it less efficiently than if you spent a little bit preparing. I was talking to a former Republican congressman, and I said, “Would you have said yes to increasing people’s taxes or increasing the deficit to fund the preparation for a low-probability event that may not occur?” And the truth is, in Republican leadership, that wouldn’t have stood a chance.
On what we can learn from New York: We learned that a hard lockdown is a critical option that has to be on the table. They did it all over Europe. They did it all over Asia. That is a much better way to get rid of the virus much more quickly. Cuomo did that. The second lesson is that when you’re the governor, you’re going to take criticism, no matter what. And there’s no way to avoid managing in a difficult situation without having people upset with you. If you communicate with people consistently and openly and honestly, then you have more permission to make tough decisions.
Tough political decisions pay off. The hard part is they don’t pay off immediately. But you put yourself in an even stronger position politically by being able to make tough decisions when there is evidence that they’re going to work. And he shows that can be done. I give Governor Abbott credit in Texas for putting in place the mask mandate. He didn’t do it as quickly as people would have liked him to—yesterday is always better than today, but today is better than tomorrow. We have governors who are learning from new information and adapting and making better decisions. I think that ought to be appreciated.
This interview has been edited for length and clarity.
President Trump pushed his desire to see schools reopen in his Wednesday evening coronavirus briefing, claiming that “a lot of people are saying” kids are unlikely to transmit the coronavirus to adults. Sorry, but the science—at least for now—isn’t saying that.
“They don’t transmit very easily,” Trump said when asked whether he was concerned that opening up schools would lead children to spread the virus to older family members. “They don’t catch it easily, they don’t bring it home easily, and if they do catch it, they get better fast.”
It’s certainly a consoling thought. But, as my colleague Jackie Mogensen recently reported, the science is still unclear. We do know, she wrote, that “children can become infected,” and it seems they tend to have milder symptoms than adults. But, she adds:
All this begs the question that’s crucial for schools in particular: If children show milder symptoms, does that mean they aren’t spreading the virus as much? That’s not totally understood, Zeichner says. “The likelihood of transmission depends on the amount of virus that somebody is producing, and the interaction of the person with the virus with the person who isn’t infected,” he says. “It is likely that children and adults with fewer symptoms may be producing less virus, which probably makes them less likely to transmit the infection.” But researchers are still investigating whether that’s the case.
And even those investigations are thorny. As our other colleague Kiera Butler wrote earlier this week, we can’t even be sure that the incubation period—the time between exposure to the virus and onset of symptoms—for kids is the same as that of adults.
Since there’s no consensus about whether children are less likely to transmit the virus to adults, there’s no consensus among public health experts about whether schools should reopen their doors to students. But that hasn’t stopped Trump from handing off the responsibility for reopening schools to local leaders while blindly hoping that the science works out. That always goessowell.
As a bonus, Trump proclaimed at the end of the briefing that he has “done more for Black Americans than anybody, with the possible exception of Abraham Lincoln.” There does seem to be a clear consensus on that one.
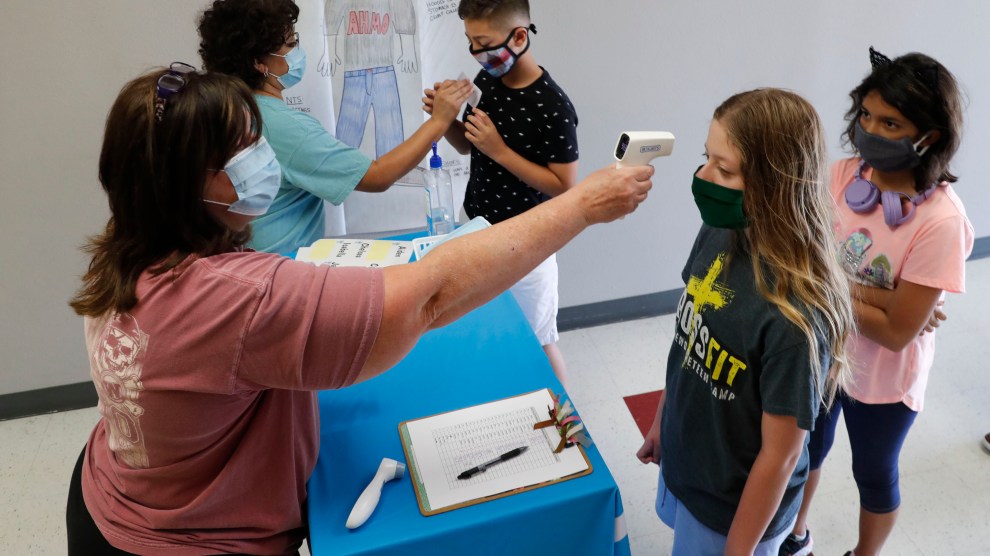
Amid concerns of the spread of COVID-19, science teachers Ann Darby, left, and Rosa Herrera check-in students before a summer STEM camp at Wylie High School Tuesday, July 14, 2020, in Wylie, Texas. AP Photo
There has been a mountain of stories written about kids, the coronavirus, and schools (including this definitively excellent piece by my colleague Jackie Flynn Mogensen). But last week, a small detail in a widely shared commentary from the medical journal Pediatrics caught my eye. “COVID-19 and Children: The Child is Not to Blame” examines studies of household transmission of the coronavirus in other countries and concludes that children rarely spread the virus to the other members of their household—usually it’s the adults whospread it to the children. It’s gotten a lot of attention. One of the authors, William Raszka, a pediatrician affiliated with the University of Vermont, appeared on a July 16 Fox News segment and advocated for the reopening of schools.
As others have pointed out, it’s tricky to compare studies of households in other countries to those in the United States because of a host of confounding variables. (Different lockdown policies! Different kinds of classrooms! Fewer mask refusers!). But let’s leave all that aside for a moment and just look at the studies themselves. This line about a study in Switzerland jumped out at me:
Of 39 evaluable households, in only 3 (8%) was a child the suspected index case, with symptom onset preceding illness in adult HHCs [household contacts]. In all other households, the child developed symptoms after or concurrent with adult HHCs, suggesting that the child was not the source of infection and that children most frequently acquire COVID-19 from adults, rather than transmitting it to them.
In other words, either a scientist orcontact tracers interviewed families that got COVID-19 and asked when each household member’s symptoms began. If the kids’ symptoms began at the same time, or after the adults, the investigators assumed that the adults caught the virus and brought it home to the kids, rather than vice versa. Chinese studies that the authors looked at relied on this same method of “symptom chronology.”
Here’s the problem: The authors’ conclusion—that children rarely bring the coronavirus home and spread it to their households—assumes that the time between exposure and when symptoms appear in children is the same as that for adults. Given that we already know that children’s immune systems seem to behave differently with the coronavirus from adults, should we accept as a given that their incubation periods are the same? I put the question to Raszka, and he reassured me via email: “To the best of our knowledge, the incubation period of the virus is the same in children as it is in adults: 2-14 days.”
But Linda Saif, an immunologist with Ohio State University and the American Association of Immunologists, had a different take. “There are just too few studies, in asymptomatic children especially, to really understand the transmission dynamics,” she wrote to me in an email.” She pointed out a Chinese paper from April that reviewed the data on children and the coronavirus. It found that children’s average incubation period was 6.5 days, slightly longer than the 5.4 day average in adults. If that’s true, Saif wrote, the findings in the Pediatrics paper “may not reflect the true transmission picture.”
I want to be careful here: It would be hasty to assume the Chinese paper is the authority on the incubation period in children. As Saif noted, there’s probably not enough research for anyone to know for sure whether symptoms appear within the same amount of time for kids and adults. Here’s what would help: Studies that rely on frequent testing of everyone in households, rather than self-reporting of when symptoms started.
Also, considering the fact that some people with COVID-19 never show symptoms at all, an epidemiologist friend pointed out that we should be doing more “seroprevalence” studies—testing people in households for antibodies to determine who actually had the virus. One such study from Spain, published earlier this monthin the medical journal The Lancet, found that children under age 10 were somewhat less likely than adults to have antibodies. That suggests that children may be less likely to acquire COVID-19 (though some people have theorized that people who don’t experience symptoms don’t make very many antibodies—and of course, antibody tests are notoriously unreliable).
Anyway, I bring all this up not to annoyingly punch holes in what seems like an otherwise reasonable commentary in Pediatrics—rather, to just point out that it is yet one more example of the crushing number of tiny details that could make a big difference in the impossible decisions facing parents, teachers, and leaders as the school year fast approaches.
As the world grapples with the devastation of thecoronavirus, one thing is clear: The United States simply wasn’t prepared. Despite repeated warnings from infectious disease experts over the years, we lacked essential beds, equipment, and medication; public health advice was confusing, and our leadership offered no clear direction while sidelining credible health professionals and institutions. Infectious disease experts agree that it’s only a matter of time before the next pandemic hits, and that could be even more deadly. So how do we fix what COVID has shown was broken? In this Mother Jones series, we’re asking experts from a wide range of disciplines one question: What are the most important steps we can take to make sure we’re better prepared next time around?
Before the pandemic, Laurel Bristow was an infectious disease researcher studying respiratory pathogens at Emory University’s Vaccine Center. In March, her lab paused its work because of the pandemic. Within days, Bristow began posting Instagram videos from her cheerful kitchen explaining the science behind the coronavirus headlines. She struck a nerve: Her account quickly grew from a few hundred to 99,000 followers. It’s not hard to see why she’s popular—Bristow deftly unpacks complex scientific concepts. She explains why critics of masks are wrong. She handily dispatches with conspiracy theories. She sheds light on the mysterious vaccine development process. She emphasizes the connection between science and the struggle for racial justice. And she does it all with millennial sass, the occasional silly filter, and cameos from her cat. Through her posts, she’s won her followers’ trust. “We’ve built social media platforms in a way that people trust individuals accounts and are more inclined to listen to what they’re saying—whether it’s right or wrong—than they are to a government agency that feels outdated and inaccessible,” she says. Bristow posts on Instagram at @kinggutterbaby.
On how her account grew: In mid-March, I had a private Instagram account with under 700 followers. It was all just people that I personally knew. My studies at work had gotten halted because of coronavirus, so I just made a post one day and said, “Would anybody be interested in knowing and understanding what’s going on with Coronavirus?” I think like 10 people said, “Yeah, I would love to hear it.” So I made my first ever front-facing video to just explain, what coronavirus is, and why we’re concerned, and why we need to flatten the curve, and what that means. People asked if I could make my profile public so that they could share it. I’m pretty sure my post said something like, Alright, I’m gonna make my profile public for 24 hours. Please don’t be horny about it and don’t send me weird DMs, strangers! I got 500 followers overnight and 2000 followers by the weekend. People just kept sending me stuff asking Can you explain this? Or what does this mean? So I just started making little videos and little stories, explaining the research that was coming out. I’ve never hash-tagged anything. I’ve never asked anyone to share my account. It has just grown from people really wanting information from someone that they feel that they can trust. Now, when I look at the stories that I’ve posted, after they’ve been out for almost a day, 20 or 30,000 people are watching them.
On the disconnect between scientists and the public: It’s been interesting to see how much my Instagram has grown. I think it highlights that there is such a big gap between the content of scientific papers and how they get translated to the public. I suspect a lot of media outlets don’t necessarily have a science writer on staff. So it causes a lot of confusion about what is fact and what is still theoretical. I think people are really desperate to have someone lay things out for them in a way that they can understand, that doesn’t feel condescending, that feels like it’s a factual summary of really complex ideas. They want to know who to trust and how to understand what makes a good research paper, as well as the limitations of specific papers, or even just of what science can accomplish right now.
It’s hard because in the age of the internet, people are so used to getting answers quickly. It’s been a big adjustment to try to understand that things are going to change as we have more information. In the beginning, the CDC told people not to wear masks, because the only thing people were thinking of were hospital grade masks, and we didn’t want to take that away from frontline workers who needed them. No one really considered the benefit of wearing cloth masks. So the recommendations changed. The difference between asymptomatic and pre-symptomatic has also caused a lot of issues with communication. People in the industry sometimes say something that is very clear to other people who are in the industry, but it’s not very clear to the public. At the same time, the public doesn’t understand that because we’re in a pandemic, some things will be reported as preliminary and then updated later. And when it gets updated, people get confused and think that they were lied to at the beginning, when the reality is, everything’s getting updated all the time.
On how she explains the pandemic to the public: I write outlines as if I’m having a conversation with someone. I was always taught that the best way to learn a subject is to see if you can teach it to somebody else. So I imagine I’m teaching a lesson, and I want to make sure that everyone can understand the concepts. I use a lot of analogies to try to convey complex scientific ideas, and people respond to that pretty well because they want it in a context that they are familiar with.
Humility and understanding go a long way. Sometimes I get DMs where people say, “Okay, you said this, I have absolutely no idea what that means.” And I have to go back and explain it. I always remind myself that when people understand science, and they understand the methods, and they understand what research is saying, they feel empowered, not scared. A lot of people right now don’t understand what’s happening, it causes them to have a lot of anxiety and feel a lot of fear about it. And that’s not how we should feel about science. Information should be empowering so that people feel like they can make smart and informed decisions for themselves and their families.
On why her approach works: People like the format that I use. They like to be able to go on social media and see a story—have someone explain something to them and spell it out. I’m not really familiar with the social media accounts of the CDC all the local departments of public health. But judging from what I saw when I worked in San Francisco on tuberculosis control for the Department of Public Health—all of these places could use a little bit of an upgrade on their social media management, because that is where so many people get their news from. If you aren’t reaching people on their level on these social media accounts, other accounts with large followings are going to fill that void. And that’s how a lot of misinformation gets spread. The organizations tasked with understanding and controlling this pandemic are putting out information, but they’re not putting it out in a way that’s accessible to people. So people are going to turn to the Instagram accounts of someone else who’s telling them in the simplest terms, oftenwhat they want to hear, which is not always the truth.
On how to make journalists better at reporting on pandemics: In the time of the pandemic, it would be beneficial for large media organizations to have a literature review class, or some kind of workshop for people who are going to cover it. They could learn, for example, what to look for when they’re reading and critiquing research papers. That goes for people who write headlines, too. Those can be a huge source of miscommunication: The article itself will say one thing, and the headline will say something that’s not entirely true, and that causes a lot of anxiety.
On battling misinformation on social media: People will say, “Oh, this person is saying this, can you address this?” And it’s hard for me—I have to resist the temptation to address those specific accounts outright, because it gives the false idea that we are equivalent. I have the vast, vast majority in the scientific community backing up what I’m saying with mountains of research, and these people have cherry-picked a few studies that are not even applicable to COVID or to recent research.
On occasion, I’ve directly referenced posts that I know that people will recognize, even if I’m not tagging the person involved. And I’ve said, “Here’s where all of this is wrong.” Because I do think it’s important to pop in sometimes and say, “Look, here’s the thing that you guys need to look for when someone’s posting stuff like this. That looks too good to be true. Here are a few key things to check in and ask yourself, is this real or is this convenient?”
On the need for science literacy education: I spend a lot of time thinking about this. Society’s perception of science for so many years was glasses and a lab coat in a lab taking care of it. The scientists are figuring it out; the scientists will take care of it. It was a very far removed thing that the public didn’t have to think about or interact with. People were okay with that for a long time. Then, as time progressed, science became more elite. It’s used a lot in advertising now, to get people to buy products without questioning. There are a lot of ads that list complex chemical interactions or claim that something boosts your immune system. But they don’t actually explain it. And the underlying feeling behind that is, don’t worry about it. It’s science. It’s too hard to understand. Just trust us.
So I think years of that combination has caused people to finally say, “Wait, I don’t know what’s happening. And I don’t know why I should trust you without understanding what’s happening.” But they don’t have the tools to understand it for themselves. It’s like a lot of other practical things that should be taught as part of the curriculum, things like how to do your taxes. You should also learn how to evaluate a scientific paper. And luckily, there are some books out there that are doing that, and they’re really fun to read. Honestly, debunking bad science is really enjoyable for me because it’s like a little treasure hunt where you figure out where they went wrong or how they’re manipulating things for their own needs, and then you get to say that you cracked the case.
This interview has been edited for length and clarity.
As the COVID-19 crisis escalates across the country, President Donald Trump is continuing to lie about the pandemic, attack his own public health officials, and insist that the virus will eventually disappear on its own.
His latest remarks—in an interview with Fox’s Chris Wallace that aired Sunday—come at a crucial juncture in the nation’s fight against the coronavirus, with cases rising in most states and death tolls once again climbing. Here are some of Trump’s most alarming, incoherent, and downright absurd lines from the interview:
“I’ll be right eventually.”
When presented with a political cartoon that was posted by a top White House communications official that mocked Dr. Anthony Fauci, Trump claimed that Fauci—one of the administration’s top infectious disease experts—was a “little bit of an alarmist.” Wallace went on to cite multiple examples of the president repeatedly assuring Americans that the virus was “under control,” that infections would soon be “close to zero,” and that at “some point” the diseases would “sort of just disappear, I hope.” Trump responded, “I’ll be right eventually.”
“I’ll say it again: It’s going to disappear—and I’ll be right,” Trump continued, before declaring that he’s “been right probably more than anyone else.”
Chris Wallace: You've been wrong a lot on coronavirus, claiming it will quickly disappear and go down to zero/
Trump: "I will be right eventually…I'll say it again, it's going to disappear." pic.twitter.com/LonHZVO8qB
Despite telling countless lies about the coronavirus, the president falsely blamed public health experts for the very false statements he himself has spread.
“Everybody thought the summer it would go away and come back in the fall, well in the summer it came,” Trump said. “They used to say the heat, the heat was good for it and really knocks it out…They got that one wrong. They got a lot wrong. The World Health [Organization] got a tremendous amount wrong. They basically did whatever China wanted them to.”
The remarks were an extraordinary attempt to distance himself from the numerous falsehoods he promoted about the virus in order to downplay its threat. “The virus that we’re talking about having to do, a lot of people think that goes away in April, with the heat, as the heat comes in, typically that will go away in April,” the president said in February, according to the New York Times. There’s evidence that hot temperatures, sunlight, and humidity kill the virus, but that hasn’t stopped it from spreading in the spring and summer months. In April, however, Trump returned to the idea, suggesting—absurdly—that doctors treat patients with “a very powerful light” or an “injection” of disinfectant.
WATCH: President Trump discusses the U.S. response to the coronavirus. Plus, his relationship with Dr. Fauci and much more. #FoxNewsSundaypic.twitter.com/JUo1c2i96Z
At one point, Trump and Wallace sparred over the rate at which the virus is killing Americans it infects, with the president repeatedly and incorrectly asserting that the United States has the “number one low mortality rate.”
Trump instructed an aide to hand Wallace a chart that would supposedly prove his point. “I hope you show this because it shows what fake news is all about,” Trump told Wallace, who quickly refuted the claim.
“The US ranked seventh, better than the United Kingdom but worse than Brazil and Russia,” Wallace explained to viewers, referring to numbers provided by John Hopkins University. Wallace noted that the White House had provided a “chart from the European CDC,” which showed “Italy and Spain doing worse [than the United States] but countries like Brazil and South Korea doing better. Other countries doing better, like Russia, aren’t included in the White House chart.”
"Ready? Will you please get me the mortality rate? Kayleigh is right here… I heard we have the best mortality rate" – the WH just flat out made up a chart to create a false impression that the US has the best mortality rate in the world during Trump's interview w/ Chris Wallace pic.twitter.com/yw8QGBTRVs
Throughout the interview, Trump repeatedly and falsely blamed increased testing capabilities for the rise in coronavirus cases.
“But sir, testing is up 37 percent,” Wallace said. “Cases are up 194 percent. It isn’t just thatthe testing has gone up, it’s that the virus has spread. The positivity rate has increased.”
“Many of those cases are young people that would heal in a day,” Trump said. “They have the sniffles and we put it down as a test…many of those cases shouldn’t even be cases.”
While it’s true that the cases among young people are rising, the president’s claim that the situation is somehow less dangerous is disingenuous, as young people are able to spread the virus to more vulnerable demographics, including elderly people and people with underlying health conditions.
“I’ll have to see.”
Stepping away from the pandemic for a moment, Trump declined to say whether he would accept the results of the November presidential election. “I have to see,” he said. “I’m not just going to say yes.”
Though he gave a similar response back in 2016, the possibility of Trump refusing a peaceful transition carries considerable more seriousness, as he’s now the incumbent.
“You couldn’t answer many of the questions.”
Trump, while bashing the competence of Joe Biden, did not appear to take well to Wallace’s assessment that the cognitive test the president recently claimed to have “aced” wasn’t all that challenging.
“Incidentally, I took the [cognitive] test, too, when I heard you passed it. It’s not the hardest test,” Wallace said. “It shows a picture, and it says, ‘What’s that?’ And it’s an elephant.”
Clearly offended, Trump shot back, “I’ll bet you couldn’t even answer the last five questions.”
It only got dumber from there:
“It’s not the hardest test. It shows a picture, and it says, ‘What’s that?’ And it’s an elephant.”
In a blistering op-ed published in the Washington PostThursday, Larry Hogan, the Republican governor of Maryland, blasted the Trump administration’s failure to recognize the threat the coronavirus posed to the United States or to formulate an adequate plan to combat it.
Hogan, who is reportedly considering a run for president in 2024, wrote that the lack of a comprehensive coronavirus response plan in the United States led him to coordinate a shipment of half a million test kits from South Korea in April—a decision for which President Trump publicly criticized him.
“I’d watched as the president downplayed the outbreak’s severity and as the White House failed to issue public warnings, draw up a 50-state strategy, or dispatch medical gear or lifesaving ventilators from the national stockpile to American hospitals,” Hogan wrote. “Eventually, it was clear that waiting around for the president to run the nation’s response was hopeless; if we delayed any longer, we’d be condemning more of our citizens to suffering and death.”
As it turned out, Maryland wasn’t able to make immediate use of the South Korean test kits because the state lacked other necessary testing components, such as nasal swabs and reagents, the Washington Post reports. Hogan’s purchase drew criticism from domestic manufacturers, who argued that the test kits he secured were not in short supply in the United States, and were available for less than he paid.
Hogan’s op-ed makes no note of the delays Maryland faced in deploying its tests, but it does note the “jarring” disparity between Trump’s flippant attitude toward the coronavirus at the beginning of the outbreak and the urgent warnings public health officials delivered to the National Governors Association in early February. “Instead of listening to his own public health experts,” Hogan wrote, “the president was talking and tweeting like a man more concerned about boosting the stock market or his reelection plans.”
Mother Jones illustration; Courtesy of Resolve to Save Lives
As the world grapples with the devastation of thecoronavirus, one thing is clear: The United States simply wasn’t prepared. Despite repeated warnings from infectious disease experts over the years, we lacked essential beds, equipment, and medication; public health advice was confusing, and our leadership offered no clear direction while sidelining credible health professionals and institutions. Infectious disease experts agree that it’s only a matter of time before the next pandemic hits, and that could be even more deadly. So how do we fix what COVID has shown was broken? In this Mother Jones series, we’re asking experts from a wide range of disciplines one question: What are the most important steps we can take to make sure we’re better prepared next time around?
Tom Frieden knows the ins and outs of the American public health system—he served as head of the Centers for Disease Control and Prevention under President Obama from 2009-2017. As the pandemic wore, he became increasingly frustrated by the red tape that held up the implementation of an effective plan. So Frieden, who now runs the global healthcare nonprofit Resolve to Save Lives, proposed a new way of funding projects that are critical to Americans’ health. In an early May hearing of the House Appropriations subcommittee on Labor, Health and Human Services and Education, Frieden introduced a funding mechanism he calls Health Defense Operations. Under this budget, pandemic response projects would be exempt from budget caps, in much the same way as the United States treats additional funding to protect its armed forces. A key part of the plan: Public health experts would be allowed to ask Congress directly for appropriate funding. “Congress and the American people must understand exactly what is needed for our public health defense so that Congress can then appropriate the resources required to sustain the public health system we need to keep us safe and healthy,” wrote Frieden in a letter to Congress in May. “This is the only way we will ensure we are prepared for the next pandemic.”
On why we need a new way to fund a swift response to pandemics: Even if you’ve got a great project, it has to do battle with every other program within an agency, and every other program within the whole government. It goes up to the larger agency like Health and Human Services and does battle with really wonderful programs like Head Start, or cancer research. And then it makes it over to the Office of Management and Budget, where some 27-year-old, who’s never run a program, makes the budget spreadsheet add up. And then it gets turned over to Congress, which pretty much ignores all of that, and bases this year’s budget on last year’s— plus or minus a little bit here or there.
We have a new idea, which is to make some of the health defense operations budget-cap exempt. That requires what’s called a bypass professional judgment, which means that the experts in an area are the ones who actually provide information on what is needed in that area. The health defense operations idea is really a new idea. We’re encouraged that we have support from a wide group, as well as bipartisan support in the House. And we’re just beginning conversations with the Senate.
On why public health agencies must be allowed to act independently of the White House: It’s naive to say, “We should insulate public health from politics.” It doesn’t happen. All public health positions have a political component. But are there ways to avoid the kind of catastrophic malfunctioning that occurred over the past few months, and that is continuing to occur here in the United States? When I look around the world, one interesting model is in the United Kingdom: They have a chief medical officer who is appointed for a term that spans administrations. You can imagine a system that appointed either the CDC director or someone else and had that individual for a five-year renewable term, so they would span administrations and, in theory, be less, less reluctant to speak out. That happens in the UK. The problem is that there are lots of things that an administration can do to someone besides tell them to be quiet. They can cut their budget, for example.
On why we need to make it easier to track people down in our healthcare system—without compromising their privacy. Fundamentally, it’s very hard to know who is who in our healthcare system. So if John Smith comes in with a COVID test that’s positive, and says he exposed eight people, it’s really hard to find him and other people. That is something that has to be addressed in a way that is entirely transparent to people and protects confidentiality and privacy, and doesn’t lead to people avoiding care if, for example, their immigration is status is not clear. We don’t have that, and it’s one of the fundamental problems in why we have trouble with infectious disease outbreaks.
On why we need to scale up our global work: This is very important. One of the things that my organization does is advocate for funding for global health security and help countries actually spend that money well—because ultimately, most of the threats will come from elsewhere. And it will be both cheaper and more effective to stop them at the source rather than wait until they get to our shores. If countries are stronger, then we’re safer here.
On the CDC: Blaming the CDC is like blaming a person who has been bound and encased in cement for failing to swim. CDC has not communicated on this well because they have not been allowed to communicate with us. And anyone who doesn’t understand that doesn’t understand how government works. CDC would have loved to be giving daily briefings with one of the top experts. And they did that. And it said exactly what was happening exactly when it was happening in exactly the right language. On January 26, Nancy Messonier said, we have to act, we have to behave as if this is a pandemic. On February 26, she said, disruption to our everyday lives may be severe. This was exactly right, exactly the right thing to say, at exactly the right time. And they were basically told to be quiet after that. So I think that the issue is not so much: “Why didn’t CDC do what it was supposed to do?” But “Why wasn’t CDC allowed to do what it could have done?”
This interview has been edited for length and clarity.
Mother Jones illustration; Courtesy of Mother Jones illustration; Boston University School of MedicineCourtesy of Boston University School of Medicine
As the world grapples with the devastation of thecoronavirus, one thing is clear: The United States simply wasn’t prepared. Despite repeated warnings from infectious disease experts over the years, we lacked essential beds, equipment, and medication; public health advice was confusing; and our leadership offered no clear direction while sidelining credible health professionals and institutions. Infectious disease experts agree that it’s only a matter of time before the next pandemic hits, and that one could be even more deadly. So how do we fix what COVID-19 has shown was broken? In this Mother Jones series, we’re asking experts from a wide range of disciplines one question: What are the most important steps we can take to make sure we’re better prepared next time around?
Nahid Bhadelia is an infectious disease physician and medical director of special pathogens unit at Boston Medical Center. For the last nine years, she has directed the medical response program for Boston University’s maximum containment biosafety level 4 lab, one of only two centers of its kind in the United States—the other one is in Galveston, Texas—equipped to study the most highly contagious and dangerous diseases. During the West African Ebola epidemic that began in 2014, she worked extensively on the ground in affected countries—in 2016, she began working with a research and patient care facility in Uganda dedicated to combating viral hemorrhagic fevers like Ebola. In addition to her work in Boston, she now helps run that facility in partnership with Ugandan doctors and scientists. She also leads a project in Liberia that trains local scientists in emerging infectious disease research.
On the importance of US infectious disease work abroad: Let’s look at the humanitarian aspect and then the selfish aspect. I think the two are related, because the way you stop outbreak clusters of infectious diseases from becoming pandemics is that you catch them early. At the tail end of all international surveillance for infectious diseases are the communities that do not have access to care. And in the majority of these settings, when people have febrile illnesses, they don’t get diagnosed. Everything just gets diagnosed as malaria. The good thing that happened after Ebola was the global health security agenda stuff, which increased investments in setting up diagnostics abroad, setting up response structures abroad, setting up surveillance, so that we get an early warning in some way. The other thing that happened in the aftermath of the Ebola epidemic was that ASPR invested a ton of money in identifying Ebola treatment centers in the United States. They invested in hospitals that are taking care of Ebola patients to make them into the National Emerging Special Pathogen Training and Education Center, a group that evaluates everybody else’s readiness. So that’s the humanitarian reason: We need to catch these outbreaks early.
Here is the selfish reason: If you want to make any headway in figuring out if a medical countermeasure or diagnostic works, you need an outbreak to evaluate these things. If you don’t have a research infrastructure in places where these outbreaks happen, when they happen, you have a really tough time setting up that research in an effective way. You won’t know if something is effective or not unless you can deploy it in an ethical way, where you can actually test efficacy. It helps the country that’s affected, and it helps us. And that’s why the Department of Defense is actually involved a lot across the board in many different interests in many different ways. They have put in an incredible amount of investment, because they recognize that interdependency between the global and the local.
On why we need to scale up hospitals: Over the last five years, all of us involved in this network of biocontainment care have seen how it’s been great to get some training and awareness and infrastructure into place. But it was an infrastructure that was looking at a disease that causes a small cluster of cases with high mortality, not a disease that causes tons of cases, but not as high mortality. A three-bed biocontainment unit is not going to help you in a case like COVID, where you have hundreds of patients coming in. At a lot of conferences, I keep saying, we may be ready for Ebola, but we’re not ready for avian influenza, which is the equivalent of what we’re seeing with COVID right now.
We need to create greater surge capacity at every level, it can’t just be at these specialized centers. It can’t be an investment during that surge, during a pandemic. It needs to be consistent. It has to be devoid of attachment to a political cycle. A small hospital should have at least the same kind of capacity to handle a surge of infectious diseases, the way a large center does. The other thing, which we have so cruelly realized through this experience, is our supply chain. When the whole world’s supply chain all of a sudden gets impacted, there’s no way to be able to resolve it in time. It requires pre-investment in maintaining the supply chain. That means repatriating the supply chain for personal protective equipment or for certain medications. For example, we saw anesthetic for ventilated patients start running out, so we had to switch to other ones. Boston’s having a big epidemic, but so is New York, and everybody’s market is affected at the same time.
On why PPE needs a major reboot: Personal protective equipment is the same stuff we’ve been using for 30-something years. It’s so uncomfortable. How do you listen to the lungs and heart of a patient when you have all this stuff on your head, and you don’t want to use the same stethoscope that’s dirty on a patient? There’s all this intricate stuff that we go through that limits the amount of time the provider can spend time at the bedside. After Ebola, a couple of models came out—there was one Hopkins model for a new sort of [PPE] suit. We try to reduce the number of things you could get to take off because it’s when people take off their personal protective equipment that they’re most likely to infect themselves. The suit basically allows you to take everything off in two steps. It was full clear-face so you could you could see the face of the patient and they could see you, hear you. And it was lightweight and comfortable. There isn’t enough commercial appeal for it. The specialized centers may think they need it, but what other regular hospitals are going to invest in it?
On why doctors aren’t ready to treat infectious diseases: The next bit is training. Infectious diseases have become so specialized and not even appreciated. We require all physicians to go through advanced life support training, even though most will never see a patient who needs it. There’s some training for infection control, like personal protective equipment, but not enough to make them feel comfortable. We, as a medical field, have to invest in making everybody else have higher levels of competency in dealing with highly communicable infectious diseases.
Why isn’t that a bigger part of every curriculum? I think we need to accept the fact that we live in an age of pandemics, that this is going to continue happening, maybe not at the same scale, but we will continue to see these types of threats because that’s the environment we’ve created. This combination of human activity and population and degradation that we’re seeing with natural reservoirs, we’re going to continue to see new diseases spill over.
On why the United States should not pull out of the World Health Organization: WHO is not a perfect organization, but it is the only international infrastructure that we currently have that creates the platform on top of which sovereign nations can collaborate, and share data and technical expertise. There is nothing else like that out there. And so, for us to pull out of that basically means that we need to depend on bilateral relationships with countries you know, or regional organizations. It’s just shooting ourselves in the foot.
This interview has been edited for length and clarity.
Can you pitch in a few bucks to help fund Mother Jones' investigative journalism? We're a nonprofit (so it's tax-deductible), and reader support makes up about two-thirds of our budget.
We noticed you have an ad blocker on. Can you pitch in a few bucks to help fund Mother Jones' investigative journalism?
This is where you come in.
We’re a nonprofit newsroom, because the truth-telling investigations we do don’t happen under corporate ownership. We get to shine a bright light into the dark corners of power and report stories other media are afraid to touch.
The essential ingredient that makes this possible? Readers like you.
We’ve got a lot of hard, consequential work to do in the weeks and months ahead, and we can’t do it without reader support. Please stand up for independent media and make a donation today.
This is where you come in.
We’re a nonprofit newsroom, because the truth-telling investigations we do don’t happen under corporate ownership. We get to shine a bright light into the dark corners of power and report stories other media are afraid to touch.
The essential ingredient that makes this possible? Readers like you.
We’ve got a lot of hard, consequential work to do in the weeks and months ahead, and we can’t do it without reader support. Please stand up for independent media and make a donation today.