Lee County Emergency Management Coordinator Lee Bowdry, right, drops off boxes full of new N-95 face masks to a medical center warehouse facility in Tupelo, Miss. United States hospitals are facing an unprecedented shortage of masks.Thomas Wells/The Northeast Mississippi Daily Journal via AP
The United States government sent nearly 17.8 tons of donated medical supplies to China—including masks and respirators—almost three weeks after the first case of the coronavirus was reported in the state of Washington.
In a press release from the State Department dated Feb. 7, the agency announced it was prepared to spend up to $100 million to assist China as the number of COVID-19 cases and deaths continued to rise there. The day the press release went out, Trump tweeted that he spoke with China’s President Xi Jinping and that China would be “successful especially as the weather starts to warm & the virus hopefully becomes weaker and then gone.”
At the time, sending supplies overseas may have seemed like the right thing to do. But it’s worth noting that this release of vital medical supplies came two days after several senators, including Connecticut Democrat Chris Murphy, offered to allocate congressional emergency funding for preventative health measures and research to ward off the virus in the United States—and President Donald Trump turned it down. “Local health systems need supplies, training, screening staff, etc…” tweeted Murphy, “and they need it now.”
Just left the Administration briefing on Coronavirus. Bottom line: they aren't taking this seriously enough.
Notably, no request for ANY emergency funding, which is a big mistake. Local health systems need supplies, training, screening staff etc. And they need it now.
Trump would go on to call the virus the Democrats’ “new hoax” and deny that it posed a risk to Americans for weeks after that.
How the tables have turned. As of Saturday afternoon, the Centers for Disease Control and Prevention reports 103,321 cases of the coronavirus in the United States and 1,668 deaths, the highest number of confirmed cases worldwide. Hospitals across the country are now experiencing an unprecedented shortage of respirators and masks. Desperate nurses and doctors are taking to social media to show their need for protective equipment with the hashtag #GetMePPE, as they treat patients who are dying of the virus.
On Wednesday, the Trump administration asked the international community for donations of equipment, including N-95 masks, gloves, respirators, and hand sanitizer. But even as his officials ask for foreign aid, as CNN points out, Trump has a very different public message. As he boasted during Tuesday’s coronavirus briefing at the White House: “We should never be reliant on a foreign country for the means of our own survival.”
Speaker of the House Nancy Pelosi (D-Calif.) told CNN’s Jake Tapper Sunday morning that Trump’s response at the beginning of the coronavirus pandemic ultimately cost American lives. “His denial at the beginning was deadly,” Pelosi said. Trump’s continuous delay in “getting equipment to where it’s needed, is deadly.”
President Donald Trump says he may announce a two-week quarantine for residents of Connecticut, New Jersey, and New York as soon as today.
“We might not have to do it,” Trump told reporters on Saturday, “but there’s a possibility that sometime today we’ll do a quarantine—short term, two weeks—for New York, probably New Jersey, certain parts of Connecticut.” Trump’s maybe-maybe-not approach is likely to only add to the chaos being caused by the new coronavirus.
WATCH: NEWS President Trump says he is considering an enforceable quarantine of hot spots in northeast to restrict travel. #coronaviruspic.twitter.com/luFfAL2vfv
Trump said travel could be restricted from the three states “because they’re having problems down in Florida”—a key swing state in the 2020 election. “A lot of New Yorkers are going down [to Florida],” Trump said. “We don’t want that.” The president said he’d spoken by phone with Florida Gov. Ron DeSantis (R), a vocal Trump supporter who has been widely criticized for his response to the pandemic.
Trump added before boarding Marine One that it would be an “enforceable quarantine,” saying, “I’d rather not do it, but we may need it.” The president followed up his quarantine comment with a similar tweet.
I am giving consideration to a QUARANTINE of developing “hot spots”, New York, New Jersey, and Connecticut. A decision will be made, one way or another, shortly.
Gov. Andrew Cuomo (D-N.Y.) said Saturday that he hadn’t spoken with Trump about the possibility of a quarantine. “I haven’t had those conversations. I don’t even know what that means,” Cuomo said at a press briefing. “I don’t know how that could be legally enforceable, and from a medical point of view I don’t know what you would be accomplishing.”
A copy of a check signed by President Donald Trump donating three months of his salary to the Department of Education.Pablo Martinez Monsivais/AP
In a move that should surprise no one, President Donald Trump reportedly wants his signature on the checks that will be sent out to many Americans after Congress passed a $2 trillion stimulus bill with overwhelming bipartisan support.
The Wall Street Journal reported Friday evening that Trump wants his name of the checks, citing an unnamed administration official. Normally, a civil servant would sign them. It’s a move that various commentators predicted in the days for the bill became law.
Prediction – if the coronavirus emergency aid checks go out, this will be the signature: pic.twitter.com/4Nd3NlQp01
The money for the checks comes from Congress, not Trump. The Senate passed the stimulus bill 96-0 on Wednesday. In the House, the bill was set to easily pass by voice vote until Rep. Thomas Massie (R-Ky.) tried to force a recorded roll call vote. Massie’s (unsuccessful) stunt forced legislators to fly back to Washington in the middle of a pandemic.
Trump responded by tweeting that Massie is “a third rate Grandstander” who “just wants publicity.” In a rare moment of Twitter harmony, John Kerry agreed with the president. “Congressman Massie has tested positive for being an asshole,” Kerry tweeted in response to Trump. “He must be quarantined to prevent the spread of his massive stupidity.”
Santa Barbara Cottage Hospital, where COVID-19 patients are being treated in Santa Barbara County, CaliforniaAmy Katz/ZUMA
When health insurance companies set premiums for 2020, they weren’t counting on a global pandemic that could potentially cost them hundreds of billions of dollars. Now a new analysis estimates that premiums could increase substantially next year if insurance companies try to recoup those costs and Congress doesn’t provide emergency assistance.
Covered California, the state’s Obamacare marketplace, explains that insurance companies set prices for the commercial plans that individuals and employers buy “well before there was even any hint of the virus.” Peter V. Lee, Covered California’s executive director, told the New York Times, “No insurer, no state, planned and put money away for something of this significance.”
How much premiums are likely to rise is still highly uncertain. Covered California estimates that the nationwide costs related to COVID-19 for commercial plans could range from $34 billion to more than $250 billion. In 2020, premiums would have been between 2 percent and 21 percent higher if those costs had been factored in, according to the analysis. If companies try to make up for the 2020 costs next year, while also budgeting for more pandemic-related spending, premiums could increase anywhere from 4 percent to more than 40 percent across the nation.
“These increased costs could mean that many of the 170 million Americans in the commercial market may lose their coverage and go without needed care as we battle a global health crisis,” Lee said in a statement that accompanied the analysis. To prevent that from happening, Covered California is calling on Congress to increase assistance to individuals who buy health insurance through individual marketplaces, and to establish a temporary program to limit the costs of COVID-19 for insurers.
Others are projecting less dramatic cost increases. Edward Kaplan, a senior vice president at Segal, a company that advises clients on health benefits, told the Times, “We think claims are really going to drop off over the next month or two.” He estimated that even in New York, the hardest hit state in the nation, health insurance costs would only increase by 4 to 5 percent.
John Bertko, Covered California’s chief actuary, argued there is an urgent need for Congress to help stabilize insurance markets. “Given that insurers will be submitting 2021 rates in May and finalizing them around July 1, congressional action is needed very soon in order to affect 2021 premiums,” Bertko said in a statement. “While there is a lot of uncertainty with anything related to COVID-19, one thing we can be certain of is that the impact will be significant, and now is the time to take action.”
President Donald Trump at a signing ceremony for a $2 trillion dollar coronavirus relief bill in the Oval Office on FridayErin Schaff/ZUMA
President Donald Trump says he plans to ignore a key oversight provision in the $2 trillion coronavirus relief bill passed by Congress this week.
The stimulus bill Trump signed on Friday afternoon creates a “special inspector general” who is supposed to notify Congress “without delay” if government agencies refuse to provide information needed to conduct oversight of the loans the administration will be doling out. In a statement released Friday evening, Trump announced he will not allow the inspector general to report to Congress without “presidential supervision.”
“I do not understand, and my Administration will not treat, this provision as permitting the [special inspector general] to issue reports to the Congress without the presidential supervision required by the Take Care Clause, Article II, section 3,” Trump wrote in a signing statement issued after he signed the bill.
The new inspector general is tasked with auditing and investigating the nearly $500 billion of loans that can be made by the Treasury Department under the new bill. Trump will appoint the inspector general, who will then have to be confirmed by the Senate.
House Speaker Nancy Pelosi (D-Calif.) told MSNBC’s Rachel Maddow Friday night that Trump’s move was “not a surprise to anyone.” She added, “Congress will exercise its oversight,” explaining that there will be a panel appointed by the House looking at the loans, as well.
Rep. Alexandria Ocasio-Cortez (D-N.Y.) took a harsher line on Twitter:
And just like that, the Congressional oversight provisions for the 1/2 TRILLION dollar Wall St slush fund (which were *already* too weak) are tossed away the day the bill is signed.
This is a frightening amount of public money to have given a corrupt admin w/ 0 accountability. https://t.co/yhL62fj58R
The use of signing statements to declare the president’s intention to disregard parts of a new law predates Trump. According to the Congressional Research Service, President George W. Bush issued signing statements challenging more than 1,000 “distinct provisions of law” across 127 different bills. CRS noted that Bush was “particularly prolific in issuing signing statements” related to, among other things, “provisions that imposed disclosure or reporting requirements.”
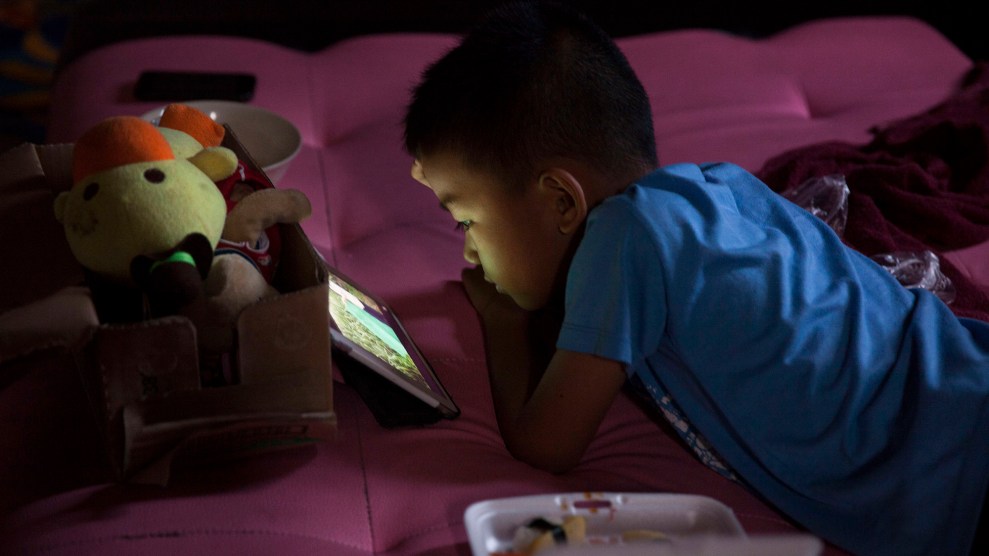
With schools shut down and residents under some kind of stay-at-home order in most states, millions of people are working from home, often with children lurking, bickering, and screaming in the background. Yet when Zoom calls are too important to ignore or we need to get through a few hours of work, we can always call upon a cheap babysitter who can endlessly enthrall our kids: streaming video.
Data from Reelgood, an app that lets users to track everything they’ve watched on streaming services such as Netflix, Hulu, and Amazon Prime, appears to confirm that more parents are relying on screens to keep homebound kids occupied. In March, its users suddenly started streaming a lot more movies and shows aimed at kids.
Reelgood’s data also shows that people are spending slightly more time on streaming services during office hours. This could be because parents are letting their kids watch TV during the day, or they could be mixing remote business with pleasure.
And who’s been virtually babysitting kids while parents let screen-time limits go and head into the unknown world of endless WFH? Some things never change: Between March 16 and 22, the top streamed kids movie was Frozen II.
This list is making me want to watch all my favorite animated movies again. (But not until I get off work.)
Residents at the Shore Towers Condominium in Astoria, New York, sing on the balcony to promote unity amid isolation measures.Ron Adar/Zuma
In late January, China’s president Xi Jinping ordered several cities to shut down in an attempt to quell the spread of a quickly moving respiratory infection we now know as the novel coronavirus. The quarantine soon included more than 50 million people. And the restrictions were stringent. The epicenter of the epidemic was in the large industrial city of Wuhan, the capital of Hubei province. In what essentially became one of history’s largest examples of a cordon sanitaire, a French term that refers to restricting people’s movement in and out of geographical areas, provincial authorities soon banned travel in private vehicles, foot police patrolled apartment complexes to keep residents indoors, and tech giants created live maps of cases using government-collected health data, prompting outcry from human rights experts.
Hubei province appears to have gotten a handle on the spread of COVID-19, the disease caused by the coronavirus, in recent weeks, and some of the travel and work restrictions have eased up accordingly. And yet, as Yanzhong Huang, a senior fellow at the US Council on Foreign Relations, wrote, “China’s harsh, restrictive containment measures are not only non-replicable in most places. They probably should not be replicated.” The draconian measures have taken a heavy toll on the society and economy there, Huang and others have argued.
The United States is not China, and President Trump continues to put the economic risks of COVID-19 above its human toll. But as the virus continues to spread—with more than 100,00 confirmed cases and 1,500 deaths—it raises the question: How much further can and should the US government intervene in individual lives in service of the public good? For insight into questions about the tensions between civil liberties and public health, I turned to Wendy K. Mariner, a professor of health law and ethics and human rights at Boston University. In 2017, Mariner co-authored a paper with her colleague Michael R. Ulrich on quarantine and the federal role in epidemics. The professors argue for a “rights-based” approach to controlling epidemics, warning that “unconstrained use of quarantines undermines both the rule of law and public confidence in government decisions in times of crisis.”
I caught up with Mariner, who is delivering the rest of the semester’s lectures remotely from her home, to understand how much authority the government has to contain us—and whether we could ever move toward the autocratic restrictions the Chinese government imposed.
Could President Trump impose a national quarantine, and what would that look like?
He has a lot of authority under many different federal statutes. Most of them are designed to provide funding in an emergency to help with disasters: the National Emergencies Act, and the Stafford Act just got invoked because of his declaration. The Department of Health and Human Services gives authority to the Centers for Disease Control and Prevention to locate people who are suspected of being infected with one of the diseases described in a presidential executive order. These are the big ones like Ebola, MERS, SARS, and this coronavirus.
We make a distinction between isolation, which usually refers to an individual, and quarantine, which tends to refer to groups—people who aren’t sick but might have a disease so we don’t want them wandering about unknowingly exposing other people.
The individual isolation is pretty straightforward in the sense that it truly is someone who’s sick. Usually it’s in the hospital where they want to be voluntarily, and that’s rarely an issue. [Forced isolation] does happen from time to time at the state level, with someone who, say, may have active contagious tuberculosis and, for one reason or another, can’t seem to take precautions, or doesn’t understand—maybe they have a developmental disability. It’s happened a few times and often with someone who’s homeless, who basically can’t stay away from other people.
At this point, couldn’t most of us be considered quarantine-able?
Well, that’s the concern, right? Who knows? This is really unprecedented. Because coronavirus appears to be transmissible before anyone knows she has it, before there are symptoms, which hasn’t been true so much in the past. This makes the lack of testing and things like that very, very troubling. We won’t know if people aren’t being tested.
We’ve seen some images from China of people locked in their apartment buildings, receiving messages from large speakers set up outside. Could our federal government lock us in our houses? What if we have no symptoms?
I think as a practical matter, no, it’s not going to do that. We don’t have a system quite like China where people are perhaps more willing to do what the government requires, as they did in the province where Wuhan is located. The Chinese government has far more coercive powers. The United States has a population that is, shall we say, somewhat more skeptical of government decisions.
But as I’ve argued elsewhere, we have to make it possible for people to stay home. And fortunately, the country is finally waking up to the notion that people do need to be able to survive both financially as well as physically. We need protections for people who don’t get paid, can’t pay the rent, lose their jobs. Gig workers, freelancers. That’s what makes it possible for people to stay home voluntarily, and it obviates the need for a government order that actually requires people to stay home.
How could a broad quarantine be enforced?
I would make a clear distinction between enforcing an individual order—an order directed to an individual or a family—and an order that would direct an entire population in a city or a state, for example, to stay home. Enforcing a single individual wouldn’t be that difficult. You could station policemen outside the home or check every once in a while to make sure that they’re not violating the orders. During the plague in other countries, notices would be put on the door: “Quarantine, stay away from this house, people inside might be infected, don’t come in.”
As a practical matter, it’s very difficult to enforce a large-scale quarantine geographically. You’re not going to line up an entire police force surrounding a city to make sure nobody goes in or out—that’s just not physically possible. It doesn’t really matter what authority you have, if it doesn’t work.
But what about using the military?
That actually might be counterproductive. And I say that because it could inflame the population who might otherwise be perfectly happy to stay home to say, “Wait a minute, we’ve got the military now coming against the civilian population.”
I think of during SARS in 2003, when the Chinese government announced that they were going to create a quarantine facility in one city and impose a geographic quarantine. Something like 250,000 people fled the city.
If you put into place measures that frighten people and make them feel as though they’re under siege, they could just bail and leave.
You write about how “shelter in place” guidelines have traditionally worked better than coercive quarantines. Do you think that’s going to be the furthest that US authorities, like mayors or governors, will go? What could be the next step?
I hope that’s as far as they have to go. If there is a case here or there of an individual not behaving smartly, the government could respond. At that point, it would probably be at the state level, because this is where most individual instances of involuntary detention occur.
But it would be hard to try and create a full cordon sanitaire that was manned by law enforcement. We don’t have enough law enforcement, and they have other important things to do.
Are there any cases that stand out in the history of the United States that have set a precedent for the government’s authority to quarantine people on a large scale?
Most examples in our history have been designed to apply to individuals on a case-by-case basis, not entire populations. So people are understandably a bit out to sea as to whether any of these laws and examples apply.
The only one that stands out was with the bubonic plague in San Francisco at the turn of the 1900s. It never got to the Supreme Court. But there was an actual quarantine around most of Chinatown in San Francisco. And it was a bit serpentine because it excluded a number of the white, or the non-Chinese, businesses. It was based in theory on the notion that people of Chinese heritage were more susceptible to the plague, which was of course nonsense.
Then a federal court struck it down, because it was a violation of equal protection. It was discriminatory, it was directed only at Chinese, and it was also arbitrary because it essentially confined people who were and were not sick in the same area, thereby encouraging the transmission of the infection, rather than preventing it.
You’ve written about how current guidelines around epidemics risk the government stepping on our constitutional rights.
Ordinarily, in order to deprive someone who has not committed a crime of physical liberty, the government would have to establish, at least with respect to contagious disease, two things: 1) the person is infected with a serious contagious disease, not just the common cold, that is easily transmitted person to person; and 2) that they are not capable of taking precautions to avoid transmitting the infection unless they are confined.
The current regulations issued under the Public Health Service Act under the authority of the HHS and the CDC have sort of ignored the second half of that. And they watered down the first by simply arguing that a person could be detained and isolated, if an official had a reasonable belief that the person was infected, period. That’s a much broader interpretation of their authority than I think the Constitution would ordinarily allow.
Now, I will give you one caveat: With a disease like COVID-19, that can be transmitted before one has symptoms, it might be reasonable to detain someone long enough to test them and see if they are in fact infected, and then see whether they take precautions and stay home and not infect anybody else. And of course, get medical care if they actually develop severe symptoms.
You wrote a paper on the role of the federal government during epidemics before the coronavirus pandemic, so I wondered if this crisis has changed your perspective in any way.
Not really. The reason is because the federal government has ability to provide the resources that are needed in a crisis like this. And I’m glad that many people in the health policy field as well as state, local, and the federal government are finally recognizing that the government should really use its authority to provide those resources, get the funding out, get the stockpiles out, release them to the public—and it should have been done weeks ago. That is going to be far more effective than locking people up.
I think it would be useful to have a more automatic trigger for things like this, like more expansive provisions for sick leave, and sick leave that allows payment for people to stay home voluntarily when they’re not sick. That’s key in this case, right? Because we’re asking people to stay home, who are not sick and don’t have symptoms.
People need to be recognized and compensated for doing the right thing, especially people who need that income and the income that they’re losing to survive financially. I’d like to see laws in place that make these kinds of personal sacrifices feasible for people. We need to have reserves in place if this kind of thing happens again. And it will.
This interview has been condensed and lightly edited.
Medical residents go over patient information with medical students.Gerald Herbert/AP
On Saturday, March 14, Avery Thompson and 650 other medical students at the University of California, San Francisco, received an email: Clinical classes were going online and planned hours in the hospital were being put on ice. The spread of the novel coronavirus posed too big a threat for courses to continue in person. In conversations with friends, she said, “We were all experiencing similar frustration at feeling like we weren’t able to do very much.” Within hours, the second-year medical student received another message. This time, from her peers. It linked to a Google Doc in which medical students and pupils from other UCSF programs—pharmaceuticals, PhD students—were drumming up ways to make themselves useful to the medical community. Within days, almost 200 students offered help, 120 from the medical school alone.
“It really just sort of snowballed,” said Hope Schwartz, a first-year medical student at UCSF. “And people started reaching out and coming up with other great ideas.” Some suggested running a blood drive; others planned to redraft public health information for the multilingual Bay Area and track down “other industries that use personal protective equipment—construction companies and nail salons.”
“Students have had the bandwidth to plan out a lot more,” Dr. John Davis, associate dean of curriculum at the medical school, said. “They mobilized immediately, as soon as Covid-19 became an issue.”
As the official number of coronavirus infections begin to skyrocket—on Monday, it was 35,000; 70,000 on Thursday, and by Friday afternoon there were over 100,000 cases—the nation’s health care apparatus has reorganized itself to face the pandemic head-on. Nonessential surgeries are being canceled, and hospitals are pleading with the public to abide by CDC recommendations of social distancing and handwashing in an effort to prevent overwhelming medical services. For medical schools, still in the middle of the academic year, clinical rotations have ground to a halt. Many instructors are too busy on the frontlines to teach, and the presence of untrained medical students could worsen supply shortages or accidentally spread the disease. Meanwhile, schools have tried to react to a quickly changing health emergency without losing sight of their responsibility to educate future doctors.
These new conditions have fundamentally changed the lives of the nation’s 30,000 medical students in two ways. First, course curriculums have reshaped themselves to fit into a world disrupted by the pandemic. Second, the coronavirus has offered students an opportunity to provide ancillary support for frontline health care workers. Across the country, students are mobilizing to meet the specific needs of the medical community in creative ways: from babysitting for nurses to 3D-printing personal protective equipment, like masks.
For many, the crisis goes to the heart of why they wanted to be doctors in the first place. “I do feel that medical students go to medical school mostly because we want be helpful,” says Orly Farber, a third-year medical student at Stanford Medical School. “We don’t write that in our essays because it’s too simplistic a reason, but it’s reality.” At Stanford, medical students are providing childcare, running errands, and going grocery shopping for the doctors and nurses whose days are fully devoted to fighting the virus. Farber thinks it’s possible their role may even be expanded by being asked to take clinical notes, make phone calls to patients, and help with orders, all tasks can be handled remotely.
In other schools, where shortages of equipment are also a concern, students are turning to technological solutions. With the materials necessary for homemade masks in short supply, students at the Rutgers New Jersey Medical School and the University of North Carolina School of Medicine have started 3D-printing face shields, which can be mass produced. “They’re cheap and easy and the most extreme thing you’d need,” says Diana Dayal, a fourth-year student at UNCSM. “If anything, we’re making the more robust product.” Some of the 170 student volunteers from UNCSM and adjacent programs are also working as “hall monitors,” helping medical workers properly “don and dox”—put on and take off—protective equipment to prevent contamination. Some Rutgers students are running a hotline at the New Jersey Poison Control Center to set the record straight for callers who’ve been inundated with misinformation about the pandemic.
For the public, even the right information can be hard to interpret. Students at the University of Pittsburgh School of Medicine are collaborating with their counterparts at New York University and the Pittsburgh Center for Autistic Advocacy to rewrite Centers for Disease Control guidelines. “We’re working as a collective effort to take these CDC guidelines and distill them down to different reading levels, so they’re accessible for a broader audience,” said Ben Zuchelkowski, a fourth-year medical student at Pittsburgh. Once the new guidelines are ready, he hopes his colleagues can disseminate them nationally.
All of the students I spoke with emphasized they could expand beyond their institutions to collaborate around the country. Across messaging applications like Slack, video-conferencing services like Zoom, and Twitter and Google Drive, students have stayed in touch: “We’re sharing ideas with each other, doing conference calls once we make a connection,” Zuchelkowski says. “It’s really been a robust organizational effort nationally.” There’s even a Google file called “Schmeddit,” where everyone can keep up to date on which programs are closed or have affiliated hospitals with confirmed COVID-19 patients.
Meanwhile, medical schools are quickly rewriting curriculums to lean on the same remote communication tools. For UCSF students, classroom courses “rapidly moved to distance and remote learning methods,” said Dr. Davis. “Those are things we could deploy quick.” It’s the same story at most other medical schools. But that’s where the similarities end. “We don’t have a nationally standardized curriculum,” he said. “Every medical school has, for all intents and purposes, its own curriculum. Each interruption in clinic and classroom activities has to be contextualized—and that’s where real complexities occur.”
Those complexities become even more fraught in the clinical setting, where students spend the majority of their third—and some of their fourth—years. Given the severity of the pandemic, clinical rotations—when students experience aspects of the profession, like surgery or primary care, in 4- to 8-week increments—have been canceled for now.
So how do you teach medical students to become doctors when their presence in a hospital is a health risk? “There’s no clear sense of how this school is going to deal with it,” said Krunal Amin, a second-year student at Duke University School of Medicine, where classes have been canceled until June 15. At UCSF, Dr. Davis said faculty members are discussing shifting clinical education from time-based to competency-based, allowing for “a bit more freedom.” In cases where that’s not possible, he’s proposed “uncoupling” courses. Instead of classroom instruction and hospital hours happening simultaneously, for instance, the first comes now, the latter after the virus subsides. Avery Thompson, the UCSF second-year, said, “They’re making the best out of a pretty bad situation, and I do appreciate that.”
Still, not everything can simply be rescheduled. Dayal says one crucial exam, which third-years take to determine where they’ll spend their first years as doctors, has been canceled.This week, most schools typically have Match Day, a celebration where fourth-years learn what that determination is. This year, celebrations moved from auditoriums illuminated in camera flash to email inboxes.
Graduation ceremonies have been canceled, but some medical schools in Boston and New York have enlisted their fourth-year students to start practicing. On Tuesday, NYU’s medical program sent out an email announcing it would graduate some of its fourth-year students three months early, so they “could join the healthcare workforce prior to the typical June 1 starting date.” New York City faces the highest concentration of infections in the country, and NYU University Medical Center is at the center of it all.
That need is trickling down to younger students, too. Last week, North Carolina’s Department of Health and Human Services—which has COVID-19 test samples but not enough technicians to process them—sought out students with lab experience who could help expedite the work. Similarly, the Allegheny County Medical Reserve Corps has reached out to students to help bolster numbers.
“I feel in the coming weeks we’re going to need backups to assist an overwhelmed healthcare workforce,” said Farber, at Stanford Medicine. “Medical students can help reinforce the frontline.”
The reality of being in the midst of a deadly pandemic, with many health care workers struggling to get basic supplies, and no clear end in sight, has created demands that are daunting to even seasoned physicians. I asked Diana Dayal, the UNCSM student, if she ever second-guessed her choice to pursue medicine. “Absolutely not,” she said. “I think it’s inspiring to have a skill set—to really be there for people at their darkest time, even if on a pandemic scale.”
On Monday, workers for the grocery delivery service Instacart are planning to strike as part of an effort for better workplace protections amid the coronavirus pandemic. The nationwide walkout is one of a handful of similaractions across the country that call attention to the few protections that exist for frontline workers putting themselves at risk. “Shoppers have had enough,” says the Gig Workers Collective in a statement announcing the strike.
“Instacart has still not provided essential protections to Shoppers on the front lines that could prevent them from becoming carriers, falling ill themselves, or worse,” the announcement says.
Instacart has said it’s hiring 300,000 new shoppers to meet the surge in demand as many Americans shelter in their homes. It has also introduced some safety measures, including paid sick leave for those diagnosed with COVID-19. But workers want more protections: hazard pay, protective equipment, and expanded sick leave.
The news was first reported by Vice. The strike is being led by Vanessa Bain, a worker in California who has been at the heart of efforts to reform Instacart—and the gig economy broadly.
SCOOP: Instacart's workers are planning a nationwide strike on Monday to protest the company's response to coronavirus.
Wildcat strikes have been sweeping the country in recent days, but this marks the first major walkout in the gig economy.https://t.co/9xKetJN4F0
An Instacart strike isn’t anything new. Back in October, I wrote about a strike Bain was organizing to fight against cut wages, unclear algorithmic pay models, and potential retaliation for their advocacy.
The coronavirus is only making those problems more glaring. Organizers like Bain have tried to use the increased visibility of workers to push change on long held concerns. But gig companies, as I reported earlier today, are doubling-down on their current employment models as their services become essential.
President Trump delivers remarks at the White House Easter Egg Roll in April 2019.Kevin Dietsch/ZUMA
Despite experts urging that quarantine measures may need to continue for months to quell the spread of coronavirus, President Trump has said he wants the United States to be “opened up and just raring to go” by Easter, in less than three weeks. Why Easter? “I think it’ll be a beautiful time,” he told reporters on Tuesday, even as the Pope was instructing bishops to help Catholics celebrate Easter from home. “Wouldn’t it be great to have all the churches full?” said Trump.
Let’s be real: Despite his recently adopted pro-life views, our twice-divorced, oft-philandering president has never been religious. What he really wants is to end the lockdown quickly in order to save “the economy.” Politicians keep suggesting we forgo public health advice and get back to work for the sake of this “economy” thing; the ironic hashtag #DieForTheDow trended on Twitter after the 69-year-old lieutenant governor of Texas suggested he’d risk dying from the virus to keep the stock market chugging. (But would he be resurrected on Easter?)
No matter what they preach in the churches of Texas, there is one authority higher than that of Jesus in this country: capitalism. In 1921, Jewish philosopher Walter Benjamin called capitalism “a purely cultic religion” that grew as “a parasite of Christianity,” until it replaced the church as the focus of Western life. Charity and selflessness are still the transcendent principles guiding people’s decisions; it’s just that they’re invoked to serve the market instead of other people.
If given the choice between dying and plunging the country I love into a Great Depression, I’d happily die. https://t.co/MznAkp3kwD
Congress limited its relief spending for American households by diverting vast sums to major industries. We can’t afford to give everyone health care, they say; better to watch people get sick and die instead of the airline industry.
This relentless focus on profit has not translated into higher wages for the average American in almost half a century. “In our world, we no longer work in order to satisfy our own needs,” writes Byung-Chul Han, a Korean-German theorist of neoliberalism, in his 2017 book Psychopolitics. “Instead, we work for Capital. Capital generates needs of its own; mistakenly, we perceive these needs as if they belonged to us.” He adds that neither workers nor the ruling class is free from these demands: “Today, the Dictatorship of Capital rules over everyone.”
Yet the privileged few—politicians, investors, corporate execs—benefit from this arrangement. They leverage stock buybacks and insider knowledge to keep their pockets flush while workers take the hit. They ask beleaguered tenants to keep paying rent and threaten to evict paramedics. When they talk about dying for “the economy,” what they really mean is you dying for their economy. God rewards His faithful servants.
Meanwhile, the World Health Organization continues stressing the need for a collaborative response to a virus that is, by its nature, a threat to the entire human species; no country or class is exempt. In a speech urging lockdown measures to stop the rampant spread, the WHO director-general said, “Let our shared humanity be the antidote to our shared threat.”
Capitalists typically justify poverty and illness by blaming groups of people: some don’t work hard enough (the “undeserving poor”); others are simply unclean. The coronavirus explodes such rationalizations. Among people stricken with the virus, there is no undeserving sick, and no amount of hard work and fiscal prudence could have saved people from economic devastation. In a pandemic, the illusions fall away, and the true nature of these everyday distinctions is exposed—it’s not the good against the wicked; it’s the market against humanity.
I’d like to think there was a time when humanity was prioritized over capital, profit, and the economy. Even today, the rapid growth of mutual aid networks responding to COVID-19 shows that plenty of us are willing to make generous sacrifices for people we’ve never met. Supporting others in your community will never be unimportant, yet many of these efforts—like Venmoing newly unemployed friends to help them pay bills—would not be necessary in countries that have woven strong social safety nets to catch their vulnerable. Every Italian, for instance, is entitled to four weeks of paid vacation per year, on top of paid sick days.
“It’s too expensive,” you can imagine our leaders saying when considering such a policy, Republican and Democrat alike. “We can’t afford it.” They’d sooner give up the sanctity of human life than reach toward a different system. Adopting single-payer health care, universal basic income, and other forms of social democracy has long been considered politically impossible in the US—until coronavirus hit. We can begin the work of re-ordering our priorities now that they’ve been laid bare.
Meanwhile, the White House Easter Egg Roll will likely remain canceled, and Trump will throw a tantrum somewhere in the White House, from deep within his social isolation.
My favorite neighborhood restaurant is effectively closed down right now, and there’s a good chance yours is, too. As an increasing number of cities and states issue shelter-in-place orders, many of these places—now legally limited to serving take-out—have made the difficult decision to suspend business altogether, citing the financially impossible combination of hefty overhead and slow sales. In many cases, that’s also meant full layoffs of their staffs.
As a human being with a heart, it’s been difficult to accept that the smiling faces of servers, bartenders, and baristas who greeted me several times a week have been replaced by furrowed brows as the newly unemployed imagine a long stretch with no paycheck—and the owners of these establishments face the prospect of financial ruin. My support for my favorite places has been limited to what’s felt like meager attempts to keep them afloat: buying gift cards for future visits and contributing to GoFundMe pots set up to benefit the workers. In the case of my neighborhood joint, I’ve also been buying up stashes of the extra coffee beans they’re selling off and baked goods they’re occasionally churning out from their kitchen.
This week, the Senate passed an emergency relief bill that included $349 billion in loans to small businesses; any amount spent on payroll, rent, or utilities would be converted into grants that do not need to be repaid. That seemed like a welcome stopgap for places like the restaurants I frequented in a pre-pandemic life. But when I went to place one of those ad-hoc bakery orders today, I was met with this protest:
The post takes aim at a section of the bill that allows big restaurant and hotel chains to take advantage of the small business relief money for any of their individual hotels and restaurants that have fewer than 500 employees. Critics argued that these big chains will take more than half of the allocated funds, leaving many smaller businesses without the cash they need to stay afloat. “Masquerading these franchisees as small businesses will pull the rug out from under independent bars and restaurants,” the post says, inviting followers to speak out against this loophole.
Other restaurants across Washington, DC, where I live, posted identical messages. When I asked one of the restaurants where the image had originated, they directed me to the DC Hospitality Coalition, whose ally organizations in Philadelphia, Chicago, San Francisco, Seattle, and New York had posted the same thing. (I reached out to the DC group; I haven’t yet received a response.)
An earlier version of the legislation had reserved the whole pot for independently owned small businesses, but Senate Majority Leader Mitch McConnell (R-Ky.) and Sen. Marco Rubio (R-Fla.) slid in the provision allowing restaurant and hotel chains could qualify. So a pot of money that was supposed to support more than 30 million small businesses and their nearly 60 million employees—which, by the way, is almost half of the entire US workforce—will now be split with companies like McDonalds, which took in a record $100 billion in sales and returned more than $8 billion to shareholders through stock buybacks and dividends last year.
To be fair, the issue is complicated. Many of the name-brand hotel and restaurant locations that will benefit from the loophole aren’t actually owned by multinational corporations but are instead run by franchisees. But couldn’t companies like McDonalds make those franchise owners and their employees whole without the help of the American taxpayer? Seems like the kind of thing that the $25 billion McDonalds doled out to shareholders over the last three years would have been good for.
On Friday, the Democratic-run House passed the Senate bill on a voice vote. Some of the House’s most liberal lawmakers—often the staunchest defenders of the little guy—have said they hope to fix some of these problems in a future relief bill they promise is in the works. (The Senate has adjourned until at least April 20, and the House is not in session, making the timing of another round of relief unclear.)
I selfishly miss spending my evenings sitting at the counter sipping coffee or a glass of wine, soaking in the twee aesthetic and fermentation-heavy menu seemingly plucked from the imagination of a Bon Appetit-reading, farmers market-buying millennial like myself. When my favorite spot reopens, I plan on holding court there to make up for lost time. But the question is, will it and others like it even be able to come back? It is an absolute insult that big corporations are cutting small businesses’ place in line.
President Donald Trump speaks about the coronavirus on March 25, 2020.Alex Brandon/AP
With almost half of US novel coronavirus deaths in New York City and 44,000 people already infected there, Governor Andrew Cuomo asked the federal government for 30,000 ventilators on Tuesday to bolster the increasingly overwhelmed state healthcare system—where supply shortages, especially in New York City, are a major concern. Thursday night, President Donald Trump, during an interview with Fox News’ Sean Hannity disagreed.
“I don’t believe you need 40,000 or 30,000 ventilators,” Trump told Hannity. “You go into major hospitals sometimes, and they’ll have two ventilators.”
By Friday morning, the tune and the villain had changed. Ventilators were now a priority, the President tweeted, while slamming General Motors for not producing what he said they promised. The automobile manufacturer had been working to strike a deal with the administration to build thousands of ventilators. In a tweet, Trump criticized the company and its chief executive, Mary Barra, for sluggishness, while appearing to invoke the Defense Production Act, the federal law that can be used to compel manufacturers to expand the production of essential materials:
As usual with “this” General Motors, things just never seem to work out. They said they were going to give us 40,000 much needed Ventilators, “very quickly”. Now they are saying it will only be 6000, in late April, and they want top dollar. Always a mess with Mary B. Invoke “P”.
Minutes later, in a second emphatic tweet, Trump demanded that General Motors revive a shuttered Ohio automobile factory that it had sold to another car company more than a year ago.
General Motors MUST immediately open their stupidly abandoned Lordstown plant in Ohio, or some other plant, and START MAKING VENTILATORS, NOW!!!!!! FORD, GET GOING ON VENTILATORS, FAST!!!!!! @GeneralMotors@Ford
General Motors’ plans to open up production of ventilator masks had been weeks in the making. Though, according to reporting from Bloomberg, delays were caused by the administration, not the car manufacturer:
GM was growing exasperated with the Trump administration because after more than a week of around-the-clock work, the carmaker and Ventec had turned an auto-parts plant in Kokomo, Indiana, into a near-ready ventilator-assembly facility. Suppliers are secured for the 700 components needed to make the machines. The automaker has even started hiring because the 300 workers on staff won’t be enough to handle the proposed volume, a person familiar with the situation said.
In fact, the Trump administration was planning to announce the partnership on Wednesday, but negotiations on pricing fell through, according to the New York Times, “after the Federal Emergency Management Agency said it needed more time to assess whether the estimated cost was prohibitive.”
Meanwhile, General Motors is already positioning itself to “GET GOING ON VENTILATORS, FAST.” It just needs the administration to decide whether it actually wants to pay for them.
Sometime in his last few days, while my dad was still conscious, I handed him the iPad my friends had sent him when he first got sick. It had been a constant companion these last 14 months. He took it to infusion appointments. To his weeklong trips to Baltimore to have chemo. He used it to keep up on the news. To watch YouTubes about home and auto repair he could no longer do. He watched history shows that, he informed me, had “terrible production values” but that held his attention, particularly when he’d become too weak to read. He FaceTimed with kids and grandkids.
His hands quivered as he pressed the biometric fingerprint reader that opened it. I took it from him and slowly picked my way through settings until I figured out how to add another fingerprint, my own.
My dad did not die of the coronavirus. He died of acute myeloid leukemia, first diagnosed at Christmas of 2018. But his final days, as we moved from hospital to home to hospice, were stalked by the virus. Every day the protocols got tighter, though not tight enough soon enough. Would we still be able to visit him? How many in the room? What if someone had come from abroad? When did each of us need to leave to get ahead of travel restrictions and home to our own families? What would happen when all the things you need to do after someone dies are upended or impossible?
So I say to you: You need to get on top of your parents’ personal information, the tools that you will need if they are hospitalized or die. And you need to do it right now.
For many of you this will require having conversations about the likelihood of death far earlier than you’d hoped. Conversations that one party or another has put off. Do not put it off a day longer. If you’re lucky, this will just prepare your family for future, more ordinary passings. But you don’t know if you’ll be lucky, and you need to be ready to manage their illness and death, probably remotely. And you’ll have far less warning than I did.
Historian Clint Smith has written eloquently about the need to interview elders, before it’s too late. Please do that. Record Zoom conversations where you ask them about family lore. And schedule and record the conversations with the grandkids, too. Be your own StoryCorps.
But I’m here to talk about the practical stuff. And this is what you need to think about.
Even if they’re safely sheltering in place, you should know the names and contact numbers of any doctors they currently see. What conditions do they have? What kinds of medications do they take, how often at what dosage, and which doctor prescribes and which pharmacy fills them? What is their Social Security number? Their VA number? Their date of birth? Where are their driver’s license and passport?
Ideally, they have a living will, which helps ease probate backlog and costs and also is a process that makes you think through a lot of end-of-life issues. But most people don’t. Do they at least have an ordinary will and an advance medical directive? If so, where are they? Particularly with the directive, get a copy; keep a copy in your phone. If the answer to either is no, you can help them use various online tools to do the basics. Here are the state-by-state requirements; here’s a general guide. A video recording of them reading their will can’t hurt, especially in the few states that still require wills be notarized. Do they have a medical power of attorney—which basically empowers family members to make decisions when they can’t? Many services offer ways to do that; here’s one. In addition to their spouse or partner, should children or other family members be added to make those decisions? (Yes.) Keep that in your phone, too.
What are their wishes regarding burial and cremation or anything of that nature, recognizing that funeral rites might be delayed indefinitely? Who are their best friends and others to keep apprised or notified after death? How do you contact them?
Which bank do they use? Which mortgage company? What bills are on autopay? What bills are paid by mail? Where is the checkbook? Is there more than one? What kind of life or long-term care or any other kind of insurance do they have? Is there a safety deposit box? Where? Is the deed to the house in it? What about the car title? What else is in it? Where are the keys?
You need account numbers and passwords for everything. EVERYTHING. Bank accounts and all the stuff I just listed. But also things you might not think about, like places where precious family photos might be: Facebook, iPhoto, any other services they use (and grandparents tend to use a lot). If you have very online parents, what are the passwords to things like Twitter? You’ll want to decide whether or not to delete accounts after you’ve scraped for photos, and you won’t have that choice without passwords.
And you need to really think through access. One person I was talking to on Twitter about these issues related that her dad had put all his accounts and passwords into a carefully assembled spreadsheet. But hadn’t given his family the password to open the spreadsheet.
Are your parents technologically savvy enough to make spreadsheets and send them to you via DropBox? If not, can you walk them through that? And if not, can they relay the most important information over the phone or via secure text? And if not even that, can they write it down in a notebook and tell you where they keep it?
Save voicemails.
If somebody ends up going to the hospital right now, for any reason, you may not be able to go with them. A phone or iPad with a charger will be key to any outside communication. They or you should put their name on the device in tape or otherwise. And wifi in hospitals even under the best of circumstances can be spotty. Talk this through ahead of time, too. “Dad, if we can’t FaceTime, we’ll send you videos via text.” Try to get a nurse to enter in the wifi password if they can’t.
When my dad first got sick, I went through a manic period of getting his home ready for convalescence, figuring out his insurance and banking, donating a wooden kayak he’d made by hand, other big stuff. (Also, I set up his new soundbar.) In the intervening months, my dad sent me and my brother information about his estate. My stepmom bought him a little book to put all his passwords in, but she wasn’t sure he’d used it. After he went into hospice I dug around until I found it. The writing was shaky, but he’d done his best. He’d even included Facebook.
As my dad became less and less responsive, my brother and I and our two stepsisters had to make agonizing decisions about when we would leave. One stepsister came in from Europe to say her goodbyes. The next day guests who’d traveled abroad were banned from visiting, and she flew back to her preschooler. When it was clear that San Francisco was going to lock down, I too made the decision to leave, to return to my own son. It is what I believe my dad would have told me to do.
Before I left, I showed my stepmom, my other stepsister, and my brother some of the highlights of all the years and years of photos he’d stored on iPhoto. My dad had worked at National Geographic as an editor for many years, and up until the end he was taking pictures of the ospreys and the creek in front of his house. And pictures of trees and flowers, much like the ones I often post to Twitter. That made me smile, as did the photos of me and my brother as sullen ’80s teens. There were digital albums full of the trips he and my stepmom took all over the world. And of course, the grandkids. “I’m going to take this back to San Francisco,” I said, “and make sure we all get copies of whatever photos we want.”
United Kingdom Prime Minister Boris Johnson on Friday confirmed that he has tested positive for coronavirus, becoming the first world leader to disclose contracting the virus.
Johnson said that he would continue to lead efforts to fight the pandemic while self-isolating at 10 Downing Street, his official residence. “I’m working from home and self-isolating, and that’s entirely the right thing to do,” he said in a video posted to Twitter.
“But be in no doubt that I can continue thanks to the wizardry of modern technology to communicate with all my top team to lead the national fight-back against coronavirus.”
Over the last 24 hours I have developed mild symptoms and tested positive for coronavirus.
I am now self-isolating, but I will continue to lead the government’s response via video-conference as we fight this virus.
The developments come as infections continue to rise throughout the country, with 11,658 confirmed cases and 548 deaths as of Friday. For weeks, Johnson had been heavily criticized for failing to take the situation seriously enough, even as the crises in Spain and Italy rapidly unfolded. But over the past week, Johnson moved to close pubs and restaurants before finally enforcing a national lockdown to curb the spread of infections.
Joe Giddens/PA Wire URN:49102726 (Press Association via AP Images)
This piece was originally published by the Center for Public Integrity, a nonprofit, nonpartisan investigative news organization in Washington, D.C.
Sue Mullins is an outdoor person. She gardens and takes her dog for long walks. But after she moved to Larimer County, Colorado, which has high ozone levels, she started running out of breath. At age 70, she was diagnosed with asthma.
Now 83, she’s staring down the coronavirus with two risk factors: age and lung troubles. For safety’s sake, she said, “basically I’m under family house arrest.”
Extra caution is an especially smart move in communities like hers. Air pollution, research shows, lowers our ability to fight off infections. It worsens reactions to viruses in people with health challenges like asthma. And it could have a pernicious effect in a pandemic.
Academics at Carnegie Mellon University and the University of Montreal who studied the 1918 influenza crisis found that U.S. cities burning more coal for electricity—a stand-in for pollution at a time with little air monitoring—had substantially more “excess” deaths than low-coal cities. Their 2018 analysis compared outcomes in 180 cities, with the top third for coal use decidedly worse off than the bottom third.
“It’s this hidden cost,” said co-author Joshua Lewis, an assistant economics professor at the University of Montreal.
A century later, most of those higher-pollution cities are in areas in the top third of the U.S. for ozone, the damaging dust known as fine particles or both, a Center for Public Integrity analysis found. That includes New York, a city with a large outbreak of COVID-19, the disease the new coronavirus triggers.
The good news is that the cities choked with coal smoke in 1918 have far cleaner air now, by many measures. The bad news: Researchers keep finding health impacts from pollution at lower levels, and air-quality disparities mean some Americans—disproportionately people of color and residents with less income—breathe worse air than others.
“We see this unequal pattern across the United States,” said Jill Johnston, assistant professor of preventive medicine at the University of Southern California. “We know this kind of air pollution can really impact people across the life course, from babies to the elderly. It’s something that’s important when we think about health, to think about air quality.”
The rate of childhood asthma in New York’s Central Harlem has been estimated at four times the national level, for instance. As the coronavirus spreads through the city, Lubna Ahmed, director of environmental health for WE ACT, an environmental justice organization in Harlem, said she doesn’t want the “vulnerable communities that are so often forgotten” to get left behind yet again.
In Philadelphia, another city in the higher-pollution group in both 1918 and 2018, residents living near the East Coast’s largest oil refinery worked for years to get that major source of air emissions shut down. In June, a corroded pipe there ruptured, officials believe, triggering a fire and explosions. Refinery owner Philadelphia Energy Solutions filed for bankruptcy protection, and the complex was bought by a company that plans to redevelop it for other uses.
But Alexa Ross, campaign coordinator at the environmental justice organization Philly Thrive, is worried that the people—many African American—who breathed toxic emissions for decades in the low-income neighborhoods near the refinery are at greater risk from the new danger at their doorsteps.
“We know that our constituency does rank in that very vulnerable category of people that are immunocompromised and already have respiratory issues in particular, but also these other health struggles that weaken your immune system,” said Ross, whose group is mobilizing to help locals get the food and other necessities that they need.
Carol White, a Philly Thrive board member who has lived for 17 years in a home about 1,000 feet from the refinery complex, is helping get the word out to people, especially in nearby senior citizen high-rises. She’s facilitating by telephone and online from her house, where she’s staying put to keep safe: She’s 60 and was diagnosed with asthma last year after a refinery fire that preceded the explosion sent her to the hospital.
“Even just talking to you,” she said, “I have to catch my breath.”
People can’t undo past exposures. But there are signs air pollution is temporarily dropping in at least parts of the country amid a falloff in vehicle traffic as more Americans stay home. That’s different from the 1918 experience, said Karen Clay, a Carnegie Mellon University economics and public policy professor and lead author of the 2018 study about that pandemic.
Economic activity went down at that time, she said, but businesses “didn’t close if they didn’t absolutely have to.”
Clay and her co-authors looked at every city of more than 20,000 people with sufficient 1918 data in their 2018 paper. In a later study, they took a broader look at that flu, finding that heavy air pollution appeared to increase deaths up to 25 percent, and that poverty and poor overall community health also had substantial effects.
The Philadelphia refinery, seen in the distance from Philadelphia International Airport.
dclerch/Flickr
Too often, pollution, low income and poor health go together, a trap that people cannot escape. After her eldest daughter began to wheeze, Columba Sainz, Arizona field organizer for Moms Clean Air Force, an environmental health advocacy group, moved her family of five away from a Phoenix neighborhood where diesel buses idled. She worries about the residents who can’t afford to get out.
“People just stay inside the house or don’t spend much time outside,” she said.
Catherine Garcia Flowers, Texas field organizer for Moms Clean Air Force, wishes the country would treat pollution and climate change with the same sense of urgency as the coronavirus. As it is, the Houston resident said, too few people make the connection between air quality and health.
“People talk about allergies,” she said. “When I say, ‘Oh, what kind of allergies do you have,’ they often say, ‘I don’t know. I just can’t breathe.’”
Kern County, in California’s San Joaquin Valley, had the nation’s highest level of fine particles on an annual average and fifth-highest level of ozone in 2018. The U.S. Environmental Protection Agency measured seven times the fine particles there as it did in Kauai County, Hawaii, which had the lowest levels of that pollutant among the roughly 550 counties with monitoring data that year. Kern’s poverty rate is more than double Kauai’s.
The entire San Joaquin Valley in central California, surrounded by mountains that hold in pollutants, has struggled with air pollution for a long time. Kevin D. Hamilton, co-director and co-founder of the Central California Asthma Collaborative, a nonprofit that provides asthma services in that area, said he keeps having to correct the assumption that bad air is only a problem for a relative few.
“Children, pregnant moms, folks that are working outside every day, … elders and people with compromised immune systems or chronic health conditions,” he said, listing off the groups considered more at risk. All are “very vulnerable to this pollution, and it’s causing their immune systems to be less responsive.”
Mullins, the Colorado resident, lived in Iowa for decades before moving back to her home state. From 1979 to 1989, she served in Iowa’s House of Representatives and saw firsthand the power constituents have when they speak up. She’s among the deluge of people who filed comments in 2018 opposing an EPA proposal to restrict its use of scientific studies in a way that would make it far harder to set stricter pollution rules.
A small barge travels down the Houston Ship Channel, with Shell’s Deer Park Refinery in the background.
Mullins, who lives in Loveland, east of Rocky Mountain National Park and about 40 miles north of Denver, said it caught her off guard that a region so well-suited for getting outdoors has a problem with its air. Oil and gas development contributes. So does traffic. And then there’s climate change: Rampant wildfires in recent years have wafted pollutants to the Front Range.
Mullins takes seriously her children’s insistence that she stay inside, but she does still need to walk her dog. She keeps a close eye on air quality and uses her inhaler before she heads out.
Last week, she called her pulmonologist to get a new prescription. For days, the line was always busy. Unnerved, she wondered if she might run out.
“It was a relief to finally get through,” she said.
Since the beginning of the coronavirus outbreak in the United States, criminal justice experts, health professionals, and prisoners have warned that the virus could easily spread through crowded and dirty jails and prisons. With cases being identified daily among inmates, including in California, Colorado, Georgia, and Illinois, calls are mounting to release the most vulnerable of America’s 2.3 million incarcerated people, including older prisoners and those with underlying medical conditions.
On Rikers Island in New York City, which locks up more than 5,000 people, the potential toll from coronavirus is already becoming visible: 75 inmates and 37 staff had confirmed COVID-19 cases as of Wednesday. An investigator for the New York City Department of Corrections died last week. Mayor Bill de Blasio announced Tuesday that the city would release 300 people with misdemeanor or nonviolent felony convictions from the jail.
It may be too late to control the Rikers outbreak, says Aaron Littman, a teaching fellow at the University of California, Los Angeles law school and former litigator for the Southern Center for Human Rights. “But,” he says, “jails and prisons across the country, especially in communities that have not been hit as hard thus far, have a closing window of opportunity to dramatically decrease harm to a lot of people.” Yet they must act now: “If they wait until there are infections in their jails and prison, it will likely be too late.”
As the public health crisis expands, Littman has been scouring state laws to determine exactly what powers officials have to release incarcerated people en masse in times of emergency or pandemic. It turns out that there are many laws that already provide longstanding, if rarely used mechanisms for doing so. I called Littman up to hear more.
I saw a viral video recently showing hundreds of inmates running away from a semi-open prison in Brazil. I guess that’s one way to decarcerate. But tell me about the legal methods.
Aaron Littman: I would describe the power to decarcerate as a mosaic. And there are lots of overlapping powers. That ranges from the beat police officer who has the discretion to issue a citation or a summons rather than arresting somebody, to a booking officer in a jail who has the discretion to cite and release somebody rather than incarcerating them, to a range of powers that different officials have to release people due to an outbreak of disease. In California, it is the chief jail physician. In Massachusetts, it is the jail or prison inspector. In Mississippi, there’s a statute that says that if any infectious or contagious disease shall appear in the vicinity of any jail, the board of supervisors of the county [or other officials] “may cause the prisoners confined in such jail to be removed to some suitable place of security, for safe-keeping, until the threatened danger shall be over.” These provisions can be used to release people to home confinement.
[In at least 13 states, the laws] specifically reference outbreaks of contagious disease—what some of them call “pestilence,” which helps us know that they’re old statutes. But in some cases, they are broader. One California provision just describes an “emergency endangering the lives of inmates.”
“Pestilence” is a word I’d never use normally. But right now, it feels biblical in a way that’s almost true to what we’re living through.
AL: It does. I’ve looked some into the history of these provisions. And they have, as far as I can tell, not been frequently used. And I think that simply reflects the world-historical nature of what’s happening. This is a moment for an emergency provision to be used—as well as the array of authority that already existed to release people who, frankly, never needed to be in jail in the first place. People who were in jail because they couldn’t make bail because they were too poor. People who have been accused of very low level crimes, urinating in public, that sort of thing.
What are some examples of authority that exists in normal times—not just in the middle of a pandemic—to release prisoners?
AL: There are a variety of other release provisions that different officials, particularly sheriffs and commissioners of corrections, have in normal times that they can use now to get as many people out of their facilities as possible. In Wisconsin, state law makes clear that a sheriff has the discretion to determine who in his or her jail is placed in home detention. There are also overcrowding release [laws] that exist in many states that allow some constellation of local actors to release people once a population cap has been met. And many of these facilities are overcrowded. In most jurisdictions, governors can grant temporary reprieves from criminal sentences that would allow prisoners to return home, and then be reincarcerated if necessary after the pandemic has passed.
What have been the most promising developments that you’ve seen so far, as far as actions that public officials have taken to get people out?
AL: The New Jersey Supreme Court’s order [releasing up to 1,000 inmates from jails] was powerful. I think the Los Angeles County Jail has has been taking this seriously and is on the way to making the population reductions that are necessary. I don’t think it’s there yet. There are examples of steps in the right direction, but I don’t think anywhere is where it needs to be. Dramatic population reductions in all facilities need to happen quickly. I think that if they don’t, a lot of people die unnecessarily.
This interview has been edited and condensed for clarity.
FILE - In this Monday, March 16, 2020, file photo, Tennessee Gov. Bill Lee answers questions concerning the state's response to the coronavirus during a news conference in Nashville, Tenn. Mark Humphrey/AP
In my home state of Tennessee, the Department of Health has made one of the most depressing asks of the pandemic: It has advised doctors and nurses to seek out swim goggles and diapers to fashion into masks.
Tennessee primary care physician Sonal Gupta recounted the low point of a webinar hosted by the department in which doctors like herself and her husband, an anesthesiologist, heard the suggestion that they “use bandannas, scarves and even diapers in place of face masks and swim goggles or safety goggles in place of eye shields,” according to the Associated Press. She says her husband has been told to wash and reuse his eye mask (under normal circumstances, he replaces a used mask with a new one frequently).
This is the same state where the governor, Bill Lee, who has been in office since the 2018 midterms, declined to issue a stay-at-home order on Thursday in spite of pleas from medical professionals in Tennessee. (Though, thankfully, severalmayorsin the state have opted to fill in the gaps.) Instead, he placed his confidence in a sing-songy rhyme that will do nothing except lodge itself in people’s minds as a meaningless earworm: “Do your part, stay apart.” Mr. Lee, this is not the eighth-grade dance, where you must leave room for the Holy Spirit during the slow songs. It’s a damn pandemic, one that is particularly dangerous in your state, where 13 rural hospitals have shuttered since 2012. Tennessee ranks in the top 10 of US states for deaths caused by all sorts of things, according to the CDC; it ranks third in flu and pneumonia deaths.
I have a dog in this fight. My parents live in Tennessee. My dad, who is and has been the sole economic provider in my family for the vast majority of my life, has to keep going to work or risk losing his job. Several times a day, I am paralyzed by the terror that rushes up through my bones into my brain that one of them will fall ill, and there won’t be a thing I can do about it. I won’t be able to get to them. I won’t be able to advocate for them effectively from afar. I do not trust the hospital they would go to for care. I have spent the past two weeks jumping every time the Google alert I have set for their county and the words “coronavirus” or “COVID-19” goes off. I have spent hours on the phone with my folks, begging them to take this seriously and to take every precaution available to them. I have watched closely as the numbers in Tennessee have ticked up to nearly 1,000 confirmed cases, knowing that there are certainly more than that. I heard the governor of Kentucky, Andy Beshear, advise his people not to go to Tennessee because of the rapid acceleration of the virus there. Only Georgia and Louisiana’s numbers lead Tennessee’s in the Southeast right now.
How can I think, how can I breathe, how can I bear to be in California, 2,000 miles away from family and from my home, when things are so royally fucked that the Department of Health is advising doctors to shield themselves from infection using diapers and swim goggles? The answer is, of course, that I have no choice.
I do, however, have a question: How in the actual hell would one MacGyver a diaper into a face mask?
In a wildly cynical turn of events, the Environmental Protection Agency has decided to broadly waive environmental law because of the coronavirus pandemic.
On Thursday, the EPA’s head of enforcement Susan Bodine sent a letter to “All Governmental and Private Sector Parties.” It amounts to a free pass for all the entities that the EPA normally regulates under the Clean Air and Clean Water Acts. That’s a huge swath of industry, including facilities like refineries and chemical plants—the same types of sites that can trigger asthma attacks—even as these plants continue to operate during the pandemic. The guidance retroactively applies beginning March 13. The memo says:
The EPA regional office will evaluate whether an applicable permit, statutory, or regulatory provision addresses the situation. The EPA’s Office of Enforcement and Compliance Assurance (OECA) will work with program offices on nationwide issues that may arise. If there is no permit/regulatory provision that addresses the situation, the EPA will work with the facility to minimize or prevent the acute or imminent threat to health or the environment from the COVID-19-caused noncompliance and obtain a return to compliance as soon as possible.
This opaque language basically means the EPA is ceding its federal authority to state offices and deferring to the polluters, even on issues that could pose an “imminent threat” to public health or the environment. Cynthia Giles, associate administrator of EPA enforcement under Obama, said in a statement, “EPA should never relinquish its right and its obligation to act immediately and decisively when there is threat to public health, no matter what the reason is. I am not aware of any instance when EPA ever relinquished this fundamental authority as it does in this memo.”
The EPA will also stop requiring monitoring, so we won’t even know what the effects of this policy will be:
In general, the EPA does not expect to seek penalties for violations of routine compliance monitoring, integrity testing, sampling, laboratory analysis, training, and reporting or certification obligations in situations where the EPA agrees that COVID-19 was the cause of the noncompliance and the entity provides supporting documentation to the EPA upon request.
Last Friday, the oil lobby American Petroleum Institute requested regulatory relief from President Donald Trump, citing concerns for workers and limited numbers of staff due to the outbreak.
Giles said Thursday’s memo “is essentially a nationwide waiver of environmental rules for the indefinite future. It tells companies across the country that they will not face enforcement even if they emit unlawful air and water pollution in violation of environmental laws, so long as they claim that those failures are in some way ’caused’ by the virus pandemic.”
Giles isn’t the only former EPA staffer who is furious. “This is an open license to pollute,” Obama’s EPA administrator Gina McCarthy, who now heads the Natural Resources Defense Council, said in an emailed statement.
A stock clerk wearing gloves refills empty shelves at Whole Foods in Santa Barbara, California.Amy Katz/ZUMA
While more than half the country’s population is now under shelter-in-place orders to fight the spread of the coronavirus, grocery and pharmacy workers are still reporting for work as essential employees. As I previously reported, Minnesota and Vermont have classified grocery workers as emergency personnel, which allows them access to free child care. Michigan is also providing child care for emergency workers, including grocery clerks. Now grocery workers are demanding that California do the same.
California’s grocery and pharmacy store workers are on the frontlines during the COVID-19 pandemic.
The California petition, launched by the United Food and Commercial Workers union, calls for Gov. Gavin Newsom to take executive action to protect grocery and pharmacy workers. The emergency protections workers are calling for include paid child care, 14 additional sick days for workers affected by COVID-19, sanitation protections like the right to wash hands every 30 minutes, and customer crowd control. A spokesperson for the California Department of Public Health wrote in an email that the department would update Mother Jones if the state issues additional guidance for these workers.
Some grocery chains have implemented new protections for workers: Kroger and Walmart, for example, are adding plexiglass partitions to protect cashiers from customer germs, and some grocery and retail outlets have also given their workers temporary raises and emergency paid sick leave. But the measures have not been consistent across the industry.
John Grant, the president of Los Angeles-based UFCW 770, said the push for the emergency personnel designation was part of a national effort “to gain a modicum of protection for those clerks who are selflessly working to hold our communities together.”
It was only a matter of time before efforts to contain the coronavirus bumped up against the Sagebrush Rebellion.
Yesterday, Idaho‘s Republican governor Brad Little issued a self-isolate order closing all nonessential businesses in the state, banning all gatherings, and ordering a halt to unnecessary travel. The order was designed to prevent the community spread of the novel coronavirus, which has infected more than 123 people in Idaho so far. But the order has already stirred up a hornet’s nest from those who aren’t inclined to follow such a directive without a fight: Namely the Bundy family and their followers in the right-wing militia movement who have engaged in armed standoffs with the federal government in the past over attempts to enforce the law.
On Thursday, Ammon Bundy, one of Nevada rancher Cliven Bundy’s 14 children, posted a video on Facebook inviting people to a public meeting in Emmett, Idaho, where he lives, to talk about the coercive measures included in the governor’s self-isolate order. He read from the 11-page document, explaining that it would prevent people from gathering, riding a scooter, or traveling around the state. What’s more, law enforcement would be empowered to issue fines or even put violators in jail.
“The last time it was illegal to meet together as a people on this land was before the Revolutionary War,” he said. “Since we won our independence, it has never been illegal to assemble as a people.” Bundy then offered a brief tutorial on First Amendment rights and Supreme Court decisions acknowledging Americans’ “natural rights” to assemble peacefully.
“It does not matter what is most safe or not, what is good or not,” he said. “Because in this case, the government does not have the right to do what they’re doing. They do not have a right to restrict you from going to church, worshiping, having meetings, or being with your family, grieving with them. They do not have that right.” He compared the state government to someone trying to steal your backpack off a park bench; if that person is too big and you can’t fight back, you can call on others in the park to help you. “That is what we are doing today,” he concluded. “We are calling on you to help protect your own backpack and the very precious stuff you have in it.”
The Bundy family made similar online appeals for support back in 2014, when they engaged in an armed standoff with federal law enforcement officers who were attempting to move Cliven Bundy’s cattle off public land near his ranch in Nevada. Cliven Bundy owed more than $1 million in federal grazing fees that he hadn’t paid in two decades. Meanwhile, his cows, which were essentially feral, were menacing locals, wandering onto a local driving range, and munching through the Mesquite community garden. Militia members and other anti-government activists came from all over the country to defend Bundy, and some took up sniper positions on highways and aimed assault weapons at federal officers around the ranch. The Bureau of Land Management eventually backed off before causing any bloodshed. The cows remain a nuisance.
Two years later, Ammon Bundy also led the 2016 armed takeover of the Malheur Wildlife Refuge in Oregon to protest the prosecution of a pair of Oregon ranchers accused of arson on public land. He was charged with a variety of federal crimes for both episodes but was acquitted in Oregon. His Nevada case ended in a mistrial because of prosecutorial misconduct. Ammon has since moved to Idaho with his wife and six children.
The Bundy family seemed at one point to have fallen in with the pro-Trump crowd, as Trump embraced some of their issues, like returning control of federal land to the states and protecting Second Amendment rights. Trump also pardoned the ranchers whose case had set off the wildlife refuge takeover. But in 2018, Ammon Bundy announced that he was breaking with Trump over his anti-immigrant rhetoric aimed at migrant “caravans” coming to the southern border. Bundy criticized Trump for stereotyping migrants as “criminals” and “gang members.”
“But what about those who have come here for reasons of need?” he said in a video he posted online. “What about the fathers, the mothers, the children, who have come here and are willing to go through the process to apply for asylum so they can come into this country and benefit from not having to be oppressed continually by criminals?”
Ammon Bundy’s break with Trump and his defense of immigrants caused a major backlash from his followers in the “patriot movement.” At the end of 2018, he announced that he was leaving the movement, and he shut down his social media accounts. But Ammon has returned to the fray, and over the past two years, he has been involved in various land fights in the west. He’s also gone on the lecture circuit, giving talks about federal overreach. Over the last month, he’s posted numerous Facebook warnings about the evils of government-imposed quarantines and now he is turning those warnings into a potential confrontation. The meeting he is calling for likely violates the governor’s ban on public gatherings, which Bundy well knows. But, as he says in the video, “We’re not in any way trying to be rebellious or even civilly disobedient. We need to discuss these matters, and to decide how and what we should accept as a people.”
Can you pitch in a few bucks to help fund Mother Jones' investigative journalism? We're a nonprofit (so it's tax-deductible), and reader support makes up about two-thirds of our budget.
We noticed you have an ad blocker on. Can you pitch in a few bucks to help fund Mother Jones' investigative journalism?
Help us finish strong.
We’re not shy about asking you to help pay for the journalism you rely on—especially now. We have until December 31 to raise $400,000 to keep our nonprofit newsroom running at full strength into 2026. We’re off to a good start, but to make our goal we need contributions from readers who have never given before—and from steadfast donors who can give again. Every gift matters. Will you help us close the gap?
Help us finish strong.
We’re not shy about asking you to help pay for the journalism you rely on—especially now. We have until December 31 to raise $400,000 to keep our nonprofit newsroom running at full strength into 2026. We’re off to a good start, but to make our goal we need contributions from readers who have never given before—and from steadfast donors who can give again. Every gift matters. Will you help us close the gap?