Yesterday, Mother Jonespublished a timeline tracking 100 days since officials confirmed the first case of the coronavirus in the United States. In the weeks since, more than 1 million Americans have fallen ill and more than 57,000 have died. President Donald Trump’s record of failure, self-congratulation, and deflection snaps into focus the moment you start scrolling.
Over at the Mother Jones Podcast, we took the opportunity to examine what bearing these first 100 days could have for Trump’s 2020 reelection prospects—and the strategies he’s using to misinform and point the finger elsewhere. Host Jamilah King asked Mother Jones DC Bureau Chief David Corn to analyze the ways in which Trump has, or hasn’t, taken responsibility for the United States’ pandemic, uncovering an all-too familiar pattern. “He is trying to blame foreign power for what it did wrong so that we don’t look at what he did wrong,” Corn says.
Jamilah King also spoke with senior reporter Tim Murphy about his reporting on how candidates are adjusting to long-distance campaigning. Murphy paints a picture of a new style of digital-only campaigning, made up of livestreams, podcasts, and social media, that has profoundly affected the campaign of presumptive Democratic presidential candidate, Joe Biden. “The campaign shut down just as he was on the cusp of making history,” Murphy said. “You can’t do the big wine cave fundraisers anymore.”
Listen to the full story on the podcast:
And while you’re here, check out our video chronicling Trump’s 100 days of denial:
At an industry roundtable on Wednesday, Trump set out to assure Americans that soon the country will reopen, the coronavirus will disappear, and things will be just as they were three months ago.
And then he took questions.
“Without a vaccine, sir, why do you think the the virus is going to be gone?” asked CBS News reporter Ben Tracy.
“It’s gonna go,” Trump responded. “It’s gonna leave. It’s gonna be gone. It’s gonna be eradicated. It might take longer, it might be in smaller sections. It won’t be what we had.” He went on, “If you have a flare-up in a certain area—I call them burning embers—boom, we put it out. We know how to put it out now.”
.@benstracy asks Pres. Trump how he expects coronavirus to be "gone" without a vaccine
Trump: "It's gonna go, it's gonna leave, it's gonna be gone, it's gonna be eradicated. It might take longer, it might be in smaller sections. It won't be what we had." https://t.co/9T8aUPjUrspic.twitter.com/mc1TqQCPMH
It perhaps goes without saying that we are a long way from “knowing how to put it out.” Yesterday, the American death toll from the coronavirus surpassed that of the Vietnam War. More than a million Americans have tested positive for the virus; less than 2 percent of Americans have been tested.
Perhaps exchanges like these are why, per the Washington Post, officials have advised Trump to stop answering questions from reporters.
Local government officials in the border city of Ciudad Juárez, Mexico, are dropping bleach water from helicopters in an attempt to eliminate coronavirus—despite health officials advising against it.
Univision reported Sunday that the city’s mayor, Armando Cavada, is having sodium hypochlorite sprayed over more than 800 acres of border neighborhoods because “it’s the same material, or sanitizer, used to disinfect operating rooms,” Cavada said—a substance that cleans “totally well.”
On Wednesday morning, the helicopter was back at it, as immigration attorney Taylor Levy pointed out on Twitter:
Helicopter circling downtown Juarez area by the Paso del Norte bridge spraying a liquid that is presumed to be some sort of disinfectant against coronavirus. Officials standing near the bridge are saying its bleach water. It got on my skin but did not burn or smell significantly pic.twitter.com/0YmZxvdfKU
After the first spray last week, a Juárez resident took to Facebook to say that family members had experienced eye irritation, coughing, and vomiting. Local health officials spoke out against the tactic. They argued there is no scientific evidence that spraying at that distance would help in the first place, Univision reported, and that it also negatively affects the city’s flora and fauna.
The first round of spraying is supposed to continue for a week and will cost approximately US$65,000, according to El Diario, a local newspaper.
While Mexico hasn’t been hit as hard by the coronavirus as other countries—there have been more than 16,700 confirmed cases and more than 1,560 deaths, including 259 and 64, respectively, in Juárez—it’s still slightly behind the US timeline. The latest government projections say Mexico will see the peak of the pandemic in mid-May.
At an industry roundtable on Wednesday, President Donald Trump once again doubled down on the claim that the state of coronavirus testing in the United States is all well and good—and that complaining about it is just a favorite media pastime.
“You don’t hear about ventilators, you don’t hear about masks, and you shouldn’t be hearing about testing—but that’s the last thing they can complain about, I guess,” Trump said. “If we do 2 million tests, they say, ‘Why don’t you do 3?’ If we do 3, they say, ‘How come you didn’t do 4?’ That’s like a dream for the media.”
"You shouldn't be hearing about testing, but that's the last thing [the media] can complain about I guess … I don't know that all that [testing] is even necessary" — Trump downplays importance of testing, which he suggests is a luxury (experts say more testing is necessary) pic.twitter.com/2eMSedp4aR
Trump blamed his administration’s response on past presidents: “We had no ventilators, or very few, from previous administrations. We became the king of ventilators.” He added, “We had old fashioned tests that didn’t work, that were really obsolete,” but, “the testing has been incredible now, to a level that nobody’s seen.” (There were no COVID-19 tests before because it’s a new virus.)
Trump praised the states that have made plans to reopen their economies, making it sound like ongoing testing is just a personal pet project for governors rather than a critical public health need: “You have some governors that love the tests. You have others that like doing it a different way, an old fashioned way, with some testing. But we’re going maximum testing.”
As of yesterday, some 5.8 million Americans had been tested for coronavirus, according to the COVID Tracking Project—less than 2 percent of the US population. More than 60,000 Americans have died of the virus.
The United States reached two grim milestones this week: more Americans have now been killed by the coronavirus than in the near two decades of US involvement in the Vietnam War. The number of infections blew through the one million mark, further cementing the country’s status as the world’s worst-hit by the outbreak.
But in Jared Kushner’s own words, “this is a great success story.”
“We’re on the other side of the medical aspect of this,” the president’s son-in-law and senior adviser said during a Wednesday morning appearance on Fox & Friends. “I think that we’ve achieved all the different milestones that are needed. The federal government rose to the challenge, and this is a greatsuccessstory.”
Kushner also mocked those worried that states were reopening too quickly—as an overwhelming number of Americans are—claiming that the “eternal lockdown crowd” has it wrong. “The reality is is that the data is on our side and President Trump has created a pathway to safely open up our country and make sure that we get our economy going,” he said.
The remarks came as a startling break from reality, with Americans continuing to die in masses while experts warn that states are woefully behind on the Trump administration’s own guidelines for lifting lockdown measures. In some ways, they appeared to echo the president’s daily briefing performances, which according to a recent Washington Post analysis, are filled with self-praise and just mere minutes acknowledging the virus’ victims.
Shortly after Kushner’s television hit on Wednesday, the bleak news continued with new statistics from the Centers for Disease Control and Prevention showing that the US death toll is likely much higher than previously known.
Jared Kushner, as the US coronavirus death toll surpasses the Vietnam War and approaches 60,000: “This is a great success story, and I think that’s really what needs to be told.” pic.twitter.com/ax6ok3cYCV
Update (4/29/2020): On Tuesday night, President Trump issued an executive order declaring that the US Department of Agriculture “shall take all appropriate action” under the Defense Production Act “to ensure that meat and poultry processors continue operations.”
On April 11, South Dakota Gov. Kristi Noem formally requested that pork giant Smithfield Foods suspend operations at its massive pork-processing plant in Sioux Falls after more than 200 workers came down with COVID-19. Smithfield ultimately complied with the plea.
But such a closure is about to become illegal: The Trump administration plans to invoke the Defense Production Act (DPA) to force meat companies to remain open during such outbreaks, Bloomberg’s Jennifer Jacobs reported on April 27, citing “a person familiar with the matter.”
The news comes amid a state of increasing chaos in the industry. At least 15 meatpacking plants nationwide are currently shuttered due to spikes in COVID-19 cases among employees, idling about a quarter of US pork output and 10 percent of beef.
“The food supply chain is breaking,” John Tyson, chairman of the board of meat giant Tyson Foods, recently stated in a full-page ad published in the New York Times, the Washington Post, and several other newspapers. Warning of impending meat shortages, Tyson called on on “government bodies at the national, state, county and city levels” to ensure that meatpacking plants “remain operational so that we can supply food to our families in America.”
Magaly Licolli, executive director of Venceremos, an Arkansas workers’ rights group that focuses on the poultry industry, said invoking the DPA to keep plants humming during an outbreak constitutes a “direct attack to our workers and their communities, knowing that the majority of them are immigrants, refugees, people of color—the most vulnerable people in society.”
When I spoke to workers at poultry plants in Arkansas and Texas for a recent piece, they reported going to their job in fear of coming down with the virus and bringing it home to their families. For many workers, social distancing is virtually impossible in a high-production modern plant, and they told me that for the first several weeks of the crisis, protective masks were scarce.
Hours before publishing her Bloomberg story, Jacobs asked Trump what steps he would take to bolster the food supply under strain from COVID-19. His answer focused on the meat industry—and in particular Tyson Foods. “He told us he will do an EO [executive order] to help Tyson Foods with a “liability” problem,” Jacobs reported on Twitter.
I asked if Trump administration taking any action to protect the U.S. food supply, on closed meatpacking plants or, say, maybe ban exports of pork. He told us he will do an EO to help Tyson Foods with a “liability” problem. Food supply is ok, he told us. pic.twitter.com/6gIB3nDJCN
It’s unclear what Trump meant by “liability.” The White House did not immediately return a request for clarification.
But here’s a theory. Already, 20 meatpacking and food-processing workers have died from COVID-19, and more than 5,000 have contracted the disease, according to the United Food and Commercial Workers International Union. What if workers and their families start suing, claiming that the companies’ practices made them sick? Already, one worker—at a Smithfield plant in Milan, Mo.—filed a lawsuit claiming management was not sufficiently protecting workers from the risk of COID-19, and demanding that it follow Centers for Disease Control and Prevention guidelines.
A president invoking the Defense Production Act to require meatpacking firms to keep their plants running during outbreaks would provide a “solid basis” for shielding the firms from suits like this, said Jennifer Zwagerman, director of Drake University’s Agricultural Law Center. She noted that Walmart was recently sued for wrongful death by the family of a worker who died from COVID-19 complications.
Especially during a national emergency, Zwagerman said, “presidents have broad authority to limit liability.”
A man in a mask stands in front of the Vietnam Veterans Memorial in Washington, DC.Caroline Brehman/CQ Roll Call/AP Images
In a solemn milestone that highlights the historic nature of the pandemic, the death toll of the coronavirus in the United States has surpassed the number of American soldiers killed in the Vietnam War.
During the decades that American troops fought in Vietnam, the US military recorded 58,220 fatal casualties. The number of Vietnamese killed was far greater; more than a million North and South Vietnamese fighters died, as did two million civilians on either side. The conflict spanned nearly 20 years and sparked anti-war protests across the United States.
By comparison, the coronavirus has killed 58,365 people in the United States since it first came to the country in January, according to data from Johns Hopkins’ Coronavirus Research Center, which includes counts of probable COVID deaths.
Update (4/28/2020): NYC Health + Hospitals started testing patients at Coler for COVID-19. LeVar Lawrence tested positive for COVID-19 the day before this article was published. He had a fever but he’s doing okay. Seventy-three patients at Coler have tested positive for COVID-19 as of April 26.
Fifteen years ago, when LeVar Lawrence was 28 years old, he was shot and paralyzed from the neck down. Suddenly unable to bathe or eat or get out of bed without help, there were many days when he asked why God didn’t just let him die. In 2013, after the first hospital he was in closed down, he was moved to Coler Rehabilitation and Nursing Care Center on the northern tip of Roosevelt Island, a skinny strip of land floating between Queens and Manhattan in New York. Established in the 1950s, Coler is a city-run, long-term care facility for people like Lawrence who require full-time medical care and rely on Medicaid or Medicare to pay for it.
At Coler, Lawrence rediscovered his childhood interest in art through the OPEN DOORS project, joining an artist collective called the Reality Poets. Using a stylus that he drives with his mouth, Lawrence creates digital art. Known within the group as “the Vartist,” Lawrence illustrated the “Wheeling and Healing” poetry anthology and takes commissions. Every weekend he goes to visit his family in Brooklyn, where he was born and raised.
But for the past month, Lawrence has been isolated in his room at Coler with two other residents. Both of his roommates started showing symptoms of COVID-19 in early April. Lawrence was stuck in his bed for five days straight, growing restless and uncomfortable. “This is like being back in jail,” he told me.
The OPEN DOORS Reality Poets at the 2019 Figment Arts Festival.
Irina Island
Unlike Lawrence, most of the approximately 480 patients at Coler are elderly, but like him, the majority are in wheelchairs. All of them are considered to be medically high-risk, with severe conditions like quadriplegia or dementia. Residents typically live four to a room and require physical help to accomplish everyday tasks, like getting into their wheelchairs or eating, which makes social distancing impossible. Lawrence cannot wear a face mask because he uses his mouth to drive his wheelchair and type with a stylus on his phone. During our conversation, incessant, hacking coughs in the background interrupted the flow. “You’re hearing everything you need to know,” Lawrence said. “It’s just been hell. Very stressful.”
Nursing homes across the United States got a glimpse of the onslaught to come when COVID-19 swept through the Life Care Center in Kirkland, Washington, in late February and early March, killing at least 37 people and infecting many more. This upscale nursing home in the suburbs of Seattle had some of the earliest reported cases of the illness in the United States, but since then, nursing homes have become particularly precarious places, where a single infection can lead to dozens of deaths among elderly residents and their caregivers. Within a week of the reports coming out of Kirkland, boxes of personal protective equipment (PPE) started arriving. Photos of Servpro disaster recovery teams show nurses in head-to-toe protective suits brandishing high-tech respirators.
This is not what happened at Coler. I spoke with heath workers and residents, many of whom were concerned about speaking with me, to try to understand what it was like to be inside one of these facilities as this crisis unfolded. What I found was that Coler during the pandemic shows what happens when an institution with neglected residents is caught in a public health catastrophe.
The arrival of the coronavirus at Coler was swift and brutal. The first case was detected in mid-March, when two long-terms residents in a women’s unit tested positive for COVID-19 and one passed away. Since then, some staff estimate that over 20 residents have died. “They’re just not testing anymore,” said Cynthia, a staff nurse who is using a pseudonym for fear she might lose her job. “They said treat them all as infectious. Residents are dying every day.” There have been five deaths in Cynthia’s unit, all of whom were showing COVID-19 symptoms; she insists that none had been tested. The NYC Health + Hospitals (NYC H+H), the city agency that runs Coler, declined to comment on the number of resident deaths, citing confidentiality for patient privacy.
“They’ve been completely non-transparent with the residents and with the families of the residents,” said Patria Frias-Colon, whose cousin is paraplegic and has lived at Coler for more than 15 years. “Part of the perception among the residents is that because they are predominantly people of color—many of them young, mostly Latino and African American men who ended up there as the result of gun violence—the administration really doesn’t care about them.”
On Monday, March 16, the day after deciding to close New York City’s public schools, Mayor Bill de Blasio held a press conference to explain how the city was going to respond to the rapidly escalating spread of the coronavirus across its five boroughs. At that time there were 464 cases, but over the next month the number of cases skyrocketed to 112,141, and confirmed deaths rose to 7,890, which turned New York into the epicenter of the outbreak, first in the US and then in the world. De Blasio listed the groups of people most at risk. “Over 50, preexisting serious conditions—diabetes, lung disease, heart disease, cancer, compromised immune system. Those individuals are in the greatest danger by far,” said the mayor, who could have been describing the demographics of Coler. “Those are the people we have to go—all of us—out of our way to protect, not let anyone sick near them, make sure they are staying in, to the maximum extent possible.”
Then de Blasio outlined the city’s plan to deal with shortages in hospitals, which included moving patients into what he characterized as unused hospital facilities like Coler. “The Coler facility on Roosevelt Island, an H + H facility that was empty, it is being immediately brought back online—350 beds.” said de Blasio. “It will be ready in approximately a week’s time.”
But Coler was not empty—almost 500 people lived there. De Blasio’s administration issued a correction after being contacted by the local cable news station Spectrum News NY1. Officials then noted that Coler would only receive overflow patients from other hospitals, not patients with COVID-19 who could potentially endanger those who lived and worked there. On March 29, NYC H+H put out a statement: “The facility can hold a total of 350 non-COVID patients.” Since Coler was not supposed to receive patients who had the disease, the staff wasn’t prioritized to receive PPE.
Roosevelt Island has a long history of dealing with epidemics, quarantines, and forced isolation. It’s the home of America’s first smallpox hospital, as well as a psychiatric asylum and a prison—all of which are now destroyed or abandoned. Coler is a sprawling brick building opened in the 1940s as a hospital and long-term care facility for low-income patients. Three wings branch off the main entrance; residents live in the A and C wings, which dart off to the right and left. The entire institution is made of about 30 units with 14 people in a unit; generally one staff member is assigned to every six or seven patients. Beset by staffing shortages for years, $4.32 million was cut from Coler’s $120 million operating budget in 2019. Now, hospitals citywide are facing $400 million in cuts in the midst of a pandemic.
Those shortages have proved deadly. Cynthia’s unit is normally staffed with five health care workers. In April, she said that number dropped to three as her colleagues started calling out of work, either because they were sick or afraid of getting infected. “They are so short on staffing,” Cynthia said, “one day I came in and I was the only nurse on my floor, caring for two units.” The shortages only exacerbate the discomfort and poor health of residents. Another nurse who asked not to be named notes, “We try our best to turn them every two or three hours so they won’t break down, but you need two people for the transfer into the chair, and two people to get them back. Right now they cannot take them out. There are too few staff.”
Even before patients from other hospitals were moved there, residents were aware of the two women who had become ill in mid-March and wondered how they could possibly have gotten infected. Cynthia said that’s when she began asking for N95 respirators and PPE, but the hospital administration told her they didn’t have any. Staff continued caring for both sick and healthy patients, lifting them out of their beds, bathing them, and turning them over—all without wearing PPE.
Two days after the residents in the A wing became sick, two residents in the C wing also tested positive for COVID-19. The Coler administration started quarantining entire units, leaving patients who were showing symptoms in the same room as those who were healthy, like LeVar Lawrence. A resident who wished to remain anonymous said that on April 10, four units in the A wing and six units in the C wing were quarantined. “It’s a lot of craziness. It doesn’t have any common sense,” the resident said of the administration’s response. “Why would you hold someone who tests positive in a unit with 50 other people? It’s going to be nothing but death.”
The administration did provide thin, paperlike surgical masks and gowns to staff if patients started showing symptoms. When residents started dying, some health workers received face shields. “I asked what happened to N95,” said Cynthia. “They said we don’t have N95. Only for nurses and doctors, not nurse’s aids.” One day, one of her patients was still healthy when she left. Four hours later, she learned that the patient had been sent to Mt. Sinai hospital and died. “A healthy patient is a dead patient in four hours. We realized we don’t know what we’re up against,” she said. “We started ripping fabric to cover our hair, making our own PPE.”
At around the same time that the first COVID-19 cases started popping up at Coler, Roosevelt Islanders were on high alert that NYC H+H might start moving overflow COVID-19 patients there. Jennilie Brewster is a Roosevelt Island resident and one of the people in charge of the Open Doors project. She’s spent a lot of time at Coler over the past four years, working closely with a handful of residents, including Lawrence, and the recreational therapy department.
Following the March 16 press conference, she immediately wrote an open letter to Mayor de Blasio in which she urged the city not to move COVID-19 patients into Coler. In response, NYC H+H issued a statement on April 8 saying it had established a new Roosevelt Island Medical Center that was separate from Coler, “with no overlap or shared space,” and “no COVID-19 patients were moved into the nursing facility.” In fact, the city had outfitted unused floors of Coler with 350 beds for these patients and named it the new “Roosevelt Island Medical Center” (RIMC).
Cynthia said RIMC is set up at least partially on the fifth floor of the C wing at Coler, and it is “not separate,” because there are shared elevators and hallways. The new staff hired to work at RIMC “come through the same doors with us, they go to the same cafeteria with us on the second floor,” she said. The space separating RIMC from Coler is so minimal that one of the new nurses got lost and wandered into Cynthia’s unit one day. The nurse asked her, “Do you have COVID here?” and Cynthia responded, “Yes.” The new nurse told Cynthia that her staffing agency had said that they don’t have COVID in the building. To which Cynthia said she responded, “That is a fat lie.”
On April 3, in an attempt to call attention to the situation, a Coler staff member posted a video to Facebook. In it, five staff nurses and nurse’s aids begged for better PPE. One of the staff members who appeared in the video confirms that they were reported to HR. If they were fired, they’d lose their pension and become ineligible for future city jobs. “Someone from management asked me, why did you do this video?” the health worker said. “I said my facility is not protecting their workers. It is wrong. We need help. They informed me that we are not allowed to speak to media or anyone outside.”
Roosevelt Island is a small town within a big city. Local residents saw the video and created a “Friends of Coler” advocacy group, collecting PPE and contacting their elected officials. “I know how under resourced, how short staffed they already were,” Brewster said. On April 16, Brewster joined Assemblymember Rebecca Seawright in Coler’s parking lot to publicly deliver hundreds of gloves and surgical masks and about 100 N95 respirators. Coler CEO Dr. Robert Hughes came out to collect the supplies but denied they were necessary, telling a New York Post reporter, “We are very fortunate, we’ve always had what we needed. This adds to our ample supply but, you know, again, we are very thankful.”
NYC H+H denies that there has been a problem with PPE at Coler. “Every clinician and staff member system-wide who needs PPE during patient care/interaction has access to it,” they said in response to a request for comment. When I asked about the staffing shortage, they replied, “Coler maintains appropriate staffing levels to provide the care required to all resident[s].” Based on what Brewster was hearing from residents and staff at Coler, she was baffled by NYC H+H’s public statements. “It seemed like they should shout from the rooftops–things are bad here,” she said, “we need masks, we need staff, bring in the marines!”
Brewster noted that Friends of Coler are still actively collecting supplies, and more orders of N95s are on the way. As of last week, nurses and doctors were receiving N95 respirators, but the nurse’s aids weren’t. “This is ridiculous,” said Cynthia. “They’re the ones on the frontlines, they do the complete care, they do the cleaning, they give the baths. They’re the ones who are the most at risk.”
NYC H+H had contracted with Krucial Staffing, a Kansas-based medical personnel staffing service, to bring in nurses from around the country to work at RIMC. Some of the nurses are now suing Krucial Staffing alleging the agency had put them in unsafe conditions without proper PPE. According to court documents, a nurse from Alabama who uses the pseudonym Wyatt Logan first visited Coler on Tuesday, March 24. According to the court filing, he realized that any nurse working at Coler “would have vastly increased chances of contracting COVID,” because they have “inadequate PPE” and they were putting patients with COVID symptoms in crowded rooms, up to four beds per room.The close quarters and lack of protective gear, Logan alleges, made it clear to him that the infection would spread among roommates and the staff taking care of them.
Brewster said that there is more transparency from the city now; NYC H+H has confirmed that they are moving COVID-19 patients into unused floors at Coler, now the “Roosevelt Island Medical Center.” But the Mayor’s initial comment that Coler is “empty” has had damaging effects. “When you say Coler is empty, and actually 500 people live there, and you don’t correct that publicly, it is denying their experiences,” Brewster said. “Coler is not empty. It feeds this mythology that Roosevelt Island is this abandoned place.”
On April 17, more than a month after de Blasio’s press conference, Roosevelt Island’s three local elected officials, Gale Brewer, Rebecca Seawright, and José Serrano, wrote a letter to Dr. Mitchell Katz, president and CEO of NYC H+H. “There have been numerous—and sometimes conflicting—accounts regarding PPE, staffing, safety of patients, and nursing home residents as the new 350-bed facility comes online,” they wrote. They requested that NYC H+H confirm the numbers of COVID and non-COVID patients that have been admitted to Coler and outline the steps they’re taking when someone shows COVID symptoms. They also requested that all residents at Coler get “tested once a week for COVID.”
Seawright’s office said there has not been a response yet from NYC H+H. But according to one long-term resident who wishes to remain anonymous, during the week of April 20 they started isolating patients showing COVID-19 symptoms and fitting nurse’s aids for N95 respirators. They also started bringing in more staff from an outside agency.
Frias-Colon acknowledged that hospitals in New York City are under intense strain and need overflow beds. But she wants to know if there were any plans for keeping Coler’s original patients safe. “The message is not that we don’t want these people there,” she said referring to the COVID-19 patients who were being moved to the facility. “If there’s space they should do it, but only if it won’t compromise the patients, only if administration or staff show that they are equipped to follow the protocols they should be following. And they’re not doing it.”
So far Lawrence hasn’t had any symptoms of the coronavirus. But mentally, he is finding it hard to keep his spirits up, stuck in his room, and sometimes in his bed, as residents around him get sick. One of his fellow Reality Poets at Coler, Roy Watson, died on April 7, at the age of 65, after testing positive for COVID-19. As someone who has grown accustomed to living largely indoors, Lawrence can offer some guidance about how to cope with the pandemic. He shared one of his poems with me:
Doctor comes in shaking his head
Telling me that I will never walk and will be stuck in the bed
Told me that I needed a trache in my neck to help me breathe
Visiting hours over
Don’t want my baby mother to leave
Then looking up in the sky asking God why
Did he save me and just didn’t let me die
At that moment he spoke and said, “You’re special to me.
I have more in store for you
Just wait you’ll see.”
I told him that I didn’t want to hear that shit
Unless he’s giving me the ability to walk
He said, “My child, I just gave you back the ability to talk!”
Now, I just gave y’all part of my life to see
I know nothing about you but now you know a little bit about me
Staff members of the Galilee Center give instructions and register new aid recipients during a food distribution event outside the Center's facility in Mecca, California.Andy Cullen/High Country News
For the past five years, Juanita*, a resident of the border town of Mexicali, Mexico, has spent the spring and summer seasons in Southern California’s Eastern Coachella Valley, picking grapes, beets, blueberries and bell peppers, and then heading north for similar work in Northern California come July, once Coachella’s daytime temperatures become unbearable—120 degrees Fahrenheit. This year, however, the 66-year-old grandmother finds herself unexpectedly idle. At the end of March, she was working only two days out of six. “They cut all of our hours,” she said, wondering just how much longer she could afford to linger here, waiting for work—and pay.
In California and across the country, agricultural businesses have remained open, classified as “essential.” The farmworkers who are still employed continue to work, despite the lack of protective gear, or unemployment benefits if they fall ill. Farmworkers are especially vulnerable given the difficulty of social distancing in the fields and the underlying health conditions, like asthma, diabetes and long-term exposure to pesticides, associated with agricultural work. Many also share housing and the buses that bring them to and from work.
Coachella Mayor Stephen Hernandez is not surprised by the furloughs. The closure of restaurants, schools and large businesses has affected farms’ bottom lines, and some can’t afford to keep their workers employed. One report, from the National Agriculture Sustainable Coalition, projects that shutdowns of non-essential businesses may cause small farms selling locally to lose up to $688.7 million. Eastern Coachella Valley is “probably another two or three weeks from plowing unsold crops into the ground, as has happened in other parts of the country, Hernandez said.
The Coachella Valley stretches 45 miles from Palm Springs to the Salton Sea. The west side’s mid-century homes draped in blooming bougainvillea and its lush green golf courses vanish as you move to the east, where many of the region’s low-wage workers reside. There, rundown mobile homes and squat abodes appear even smaller against the vast desert and intermittent fields and orchards, which produce 95 percent of the country’s dates and nearly a billion dollars in fruits, vegetables, and other agricultural products.
The western valley is “a place where presidents go to retire,” said Anna Lisa Vargas, a lifelong Coachella Valley resident and community organizer. In the eastern valley, on the other hand, some residents still lack paved roads, sewage systems and municipal water—creating “a Third World within a First World.”
Over 97 percent of Eastern Coachella Valley’s roughly 147,500 residents are Latino, compared to 69.5 percent in Coachella Valley overall, and an estimated 14 percent in the unincorporated communities are undocumented. About a quarter are farmworkers, while another 40 percent work in low-paying jobs in the food, health-care and service industries. Up to half of the eastern valley’s residents live below the federal poverty line, with people in the unincorporated communities making a median income of just $18,700. Foreign-born residents, who work in the fields at higher rates, earn up to a median of $3,000 less.
Even before the pandemic, many lived “paycheck by paycheck,” said Gloria Gomez, the co-founder and executive director of the Galilee Center, a nonprofit located in Mecca. Galilee provides food, clothing, shelter and cash assistance to the area’s neediest residents, many of whom are seniors who still work in the fields, despite their increased risk of contracting the coronavirus. To survive, they have to work, she said. Since December 2017, the Galilee Center has also operated a migrant shelter that accommodates between 75-100 workers nightly. For $5 a night, workers have access to a clean bed, shower, air conditioning, WiFi and three meals a day. Still, Galilee is unable to accommodate everyone, and during the height of the harvest season, some 50 farm workers still sleep on the packed earth of the vacant lot across the street, as they have for decades.
This year, Galilee will be able to house even fewer migrants owing to social distancing guidelines: When beds are placed six feet apart, the shelter can provide only 30 of them. The shelter has set up a separate isolation area for anyone who exhibits COVID-19 symptoms; other preventive measures include temperature and symptoms checks at the door, an earlier curfew, rotating shifts for staff members to limit the number of people in the office, and a full cleanup of the facilities every two hours. “We’re concerned,” Gomez says, “but we’re here to serve,” so she has no plans to close.
The demand for Galilee’s services, meanwhile, has gone up. Its food distribution, which, by early April, had moved to car-only, is now held only once a week to limit the number of large gatherings. Galilee has gone from giving out 250 food baskets before COVID-19, to 700. Even so, it cannot meet the demand.
At first, the coronavirus seemed to be targeting the geographically more mobile communities of the west. But by early April, that trend had reversed, with over half a dozen agricultural workers at a date packinghouse in the Eastern Coachella Valley testing positive. “We know it (the coronavirus) is going to happen at one point or another, but up to right now, we (at the center) have no symptoms,” Gomez said in April. Gomez adds that the center has seen an increase in requests for help in paying rent, utilities and even diapers. At the same time, its own finances are increasingly precarious, with donations dropping 50 percent in March alone. Special COVID funds have helped, however, including a grant from the Desert Healthcare District, while continuing emergency assistance funds have kicked in for one of its partners, the FIND Food Bank.
With the coronavirus entering her community, Dominga, a 20-year resident of Mecca, an unincorporated community in the Eastern Coachella Valley, doesn’t want to go into the fields. Not working is not an option, however. The37-year-old mother of three daughters has worked an average of four or five days, out of a six-day work week, planting and picking red bell peppers, since the coronavirus hit. “We’re only 24-26 people working two fields together, when before just one field needed around 30-32 people,” she said. “With so many people that are unemployed right now, I tell myself that I’m fortunate to be working. I have my daughters, and every day I think about them when I leave.”
Note: Some names have been changed in order to protect sources with undocumented status.
Mother Jones illustration; California Historical Society; Getty
An occasional series about stuff that’s getting us through a pandemic. More here.
A few years ago, I discovered my great-great-grandmother’s home remedy book. In the mid-1860s, she had started filling a ledger with handwritten notes and newspaper clippings about fixes for household problems and treatments for a wide range of ailments. The entries, tabbed alphabetically, covered everything from ants to warts. Most of the maladies listed were common bothers—back pain, chapped lips, chest colds, chilblains, dyspepsia, earaches, flatulence, freckles, mosquito bites, nose bleeds, poison oak, toothaches, sleeplessness. The remedies, wacky and unscientific, were variously described as “perfect,” “sure,” and “excellent.”
To relieve a sore throat, the book recommends “salt pork or fat bacon sliced & simmered in hot vinegar, applied to the throat as hot as possible.” One all-purpose formula promises “to remove Grease spots from any thing & to kill Bed bugs.” A doodle of a hand points to this emphatic entry: “Also!! I have used powdered charcoal dusted on a scraped Potatoe [sic] and found it the most wonderful remedy to sooth a burn.”
While herbal ingredients abound, the recipes routinely call for less wholesome substances like borax, saltpeter, paregoric, and caustic potash. Black teeth? Brush them with honey and muriatic acid. Poor appetite? Try quinine mixed with strychnine. A sure remedy for “low spirits”: Lavender water and hartshorn, an aqueous solution of ammonia.
Don’t try this at home. Courtesy of the California Historical Society
The other day, I looked at the book again, and a few entries I’d previously overlooked popped out. Alongside the everyday nostrums are treatments for potentially deadly conditions like whooping cough and scarlet fever. There’s “a sure cure for diphtheria” and clippings suggesting ways to alleviate smallpox. An intricate “East India cure for cholera” is written out by hand, a dried leaf still pressed against its margin.
I do not know if my great-great-grandmother had occasion to try any of these, but she had good reason to keep them at hand. When she was 9, her family had sailed from Tasmania to San Francisco, only to have their prospects dashed when her father died from dysentery. (The drinking water in Gold Rush-era San Francisco was a bitch.) Throughout the late 19th century the city experienced bouts of cholera, smallpox, and bubonic plague.
Keeping a remedy book was an act of self-defense, a bulwark against the terrors of a world without germ theory or antibiotics or childhood vaccines. The earliest entries in my great-great-grandmother’s remedy book coincide with the 18-month period in which her first two children died in infancy.
Life was uncertain, death was arbitrary. That feeling of vulnerability does not seem so alien at this moment.
The impulse to shore up our psychological defenses against the unknown is particularly acute right now. Our tabs, feeds, chats, and inboxes have become digital remedy books where we collect and exchange the latest tidbits of information that might shield us and our families from infection. Should we stand 6 feet apart—or 9… or 20? What kind of mask should I wear? Should I quarantine the groceries? Disinfect the mail? Prophylactically nuke the takeout pad thai? Maybe a little gargling, zinc, elderberry, or CBD wouldn’t hurt…
You can see how an ounce of prevention can snowball into a ton of hooey. Some of the bogus notions currently out there—like bathing in Clorox to kill the virus—sound as if they came straight out of the 19th century. (The remedy book recommends sponge baths of carbolic acid to cure smallpox and scarlet fever.) No one embodies the desperation for a miracle COVID-19 cure more than the president. Hydroxychloroquine! Injecting disinfectant! Damn the double-blind testing and unfortunate side effects, what have you got to lose?
Trump’s magical thinking has made him a laughingstock. The cluelessness that suffuses my great-great grandmother’s remedies is of a different, forgivable kind. While her generation had abandoned the heroic medicine of the recent past, with its purges and bloodletting, it was still grasping at a scientific understanding of health. She was living on the cusp of an era of discovery; she just didn’t know it. While her remedy book’s unintentional goofiness still entertains me, I find its sense of resolve reassuring. We don’t really knowwhat the hell is going on, but we’ll do our best until we get there.
In case you were wondering: My great-great-grandmother, Emma Burke Gilson, beat the odds. She died when she was 80, having outlived eight of her nine siblings and surviving the 1918 flu pandemic. I wonder if she attributed her longevity to an occasional dose of honey and ginger mixed with freshly shaved iron filings—”An excellent Tonic for the Blood.”
“An excellent Tonic” Courtesy of California Historical Society
Vice President Pence answers questions during Monday's daily briefing from the coronavirus task force.Win McNamee/Getty
During Monday’s White House press briefing on coronavirus, a reporter asked Vice President Pence to explain the discrepancy between the number of tests he’d promised would be available mid-March—4 million—and the number of tests that were actually done by that time, a much lower figure. The United States did not reach its goal of conducting 4 million tests until April 20. (By contrast, a plan developed by a Nobel Prize–winning economist and a former FDA chief suggests the US should be testing 3 million people per week before re-opening even parts of the economy.)
Pence responded by claiming 4 million tests were conducted by early April, but a lag in processing the tests made the numbers seem lower.
“So when you said 4 million tests, you were talking about tests being sent out, not actually completed?” asked the reporter.
“Precisely correct,” said Pence.
Reporter @jonkarl reiterates promises made by Pence and the Trump administration for testing and Pence says "it represents a misunderstanding" by the public regarding a test and the ability to test.
The spin continued throughout the press conference. The briefing began with the leaders of CVS, Walgreens, and Rite-Aid taking the podium to reflect on the ways in which the private sector has stepped up to fight the virus. Yet it’s been more than six weeks since Trump brought these same company heads to a press conference to promise that they would scale up drive-through testing across country to meet the massive demand. Today, only 43 sites are operating in less than two dozen states, according to CNBC.
And more promises were made: President Trump today claimed that private sector partnerships would deliver more than 8 million tests in May. CVS promised 1,000 testing sites across the US by that time. Trump said by then we’ll be doing 100,000 tests per day.
Whatever justifies re-opening the states and putting people back to work. “We want them all to do it as quickly as possible,” said Trump.
Secretary of Defense Mark Esper speaks alongside President Trump. Alex Wong/Getty
Ten Senate Democrats are blasting the Defense Department’s response to the coronavirus crisis, criticizing leaders in a letter released Monday for a “slow and disjointed response” that left troops at risk.
“Civilian leadership of the Department has failed to act sufficiently quickly, and has often prioritized readiness at the expense of the health of servicemembers and their families,” the letter stated. “This failure has adversely affected morale, and, despite the Department’s best intentions, undermined readiness.”
The letter, which was addressed to Secretary of Defense Mark Esper, faulted him for “dysfunctional decision-making” that slowed the Pentagon’s response in the early days of the crisis. Among the senators’ chief concerns were Esper’s directive to overseas military officers urging them not to stray from “President Trump’s messaging” on coronavirus; his handling of the outbreak on board the USS Theodore Roosevelt, which led to the firing of the ship’s captain and the eventual resignation of the acting Navy secretary; and his decision to shield data about COVID-19 infections at military bases and installations from the public.
Since the pandemic has made regular congressional hearings all but impossible, lawmakers have scrambled to enact some form of oversight as the machinery of government responds to the crisis. The Senate Armed Services Committee attempted to hold “paper hearings,” where senators submitted questions for military leaders in writing, but shelved the idea earlier this month over what committee spokesperson Marta Hernandez said was “the additional burden on the Department of Defense at this critical time.”
Monday’s letter—which was spearheaded by Sens. Elizabeth Warren (D-Mass.), Kamala Harris (D-Calif.), and Mazie Hirono (D-Hawaii)—signals how deeply dissatisfied Democrats are with the Pentagon’s actions. While progressives have not been shy about criticizing the Defense Department, the inclusion of more moderate signatories like Sens. Amy Klobuchar (D-Minn.) and Sherrod Brown (D-Ohio), is particularly noteworthy.
The senators charged that in crafting policy for the department, Esper seemed to contradict his statement from March that his “number one priority remains to protect our forces and their families.” Generals at military bases in Italy and South Korea have been praised for their quick reactions to the spreading virus and credited with limiting infections among US personnel. But other parts of the military have been much slower to grasp the severity of the crisis.
On the Roosevelt, one of at least four aircraft carriers that has battled a coronavirus outbreak, the Navy suffered an embarrassing public relations debacle after the ship’s captain, Brett Crozier, was relieved of command when he drew attention to the worsening conditions on the ship. The Navy declined the captain’s request to quarantine most of the infected sailors in Guam, where the ship has been stationed, but eventually agreed to clear most crew members off the ship. The fiasco—which included a bizarre episode in which the Navy’s civilian leader traveled to Guam and crudely defended his decision to fire Crozier—reflected poorly on Esper, who acknowledged at the time that he had not read Crozier’s letter and was “going to rely on the Navy chain of command to go out there to assess the situation.” More than 800 Roosevelt crew members, including Crozier, have now tested positive for the virus, and one sailor has died. A Navy investigation last week concluded with the recommendation that Crozier be reinstated; Esper has not yet decided whether he will heed that suggestion.
Esper’s more recent comments about the Roosevelt “suggest a dangerous misunderstanding of the nature of COVID-19,” the senators wrote. During an interview on NBC’s Today show several days after the Navy secretary stepped down, Esper said the Roosevelt case “revealed a new dynamic of this virus, it can be carried by normal, healthy people who have no idea whatsoever that they’re carrying it.” Esper was describing asymptomatic transmission of the virus as if it were a surprising discovery, neglecting to mention that this aspect of the virus had been widely understood for weeks. “It is essential that Department leadership understand and act on the most recent and thorough understanding of the virus,” the senators wrote.
New York's Sixth Avenue is nearly free of cars in mid-April.Richard B. Levine/Levine Roberts/ZUMA
Residents of New York City, the nation’s coronavirus hot spot, will soon be able to walk, run, skate, and bike on the city’s already vacant streets. Mayor Bill de Blasio announced Monday that he was committed to closing 40 miles of streets to cars in May, with the goal of 100 total miles of street closures, to allow New Yorkers more space to socially distance outside.
Earlier in the month, the mayor’s pilot program to close a mere mile and a half of streets failed because, according to de Blasio, there were not enough NYPD officers to enforce it. After Oakland launched a program to close nearly 10 percent of its streets to cars with little police enforcement, de Blasio insisted the approach would never work in New York, saying, “We are just profoundly different than those other cities.” That same sense of New York exceptionalism is what caused the governor and mayor alike to throw up their hands and blame the city’s staggering coronavirus death toll on population density, rather than their own failure to shut things down sooner.
The street closures, mostly located in and around parks, will allow much-needed space for outdoor recreation in a city where miles of sidewalks are too narrow for social distancing. Here’s hoping that the specific street closures, when announced, actually benefit the crowded and low-income neighborhoods that need them most.
Long beforeNew Mexico or Wyoming identified any cases of COVID-19, even before residents began hoarding eggs and sacks of flour, state budgets were feeling the impact of the disease.
In mid-January, when the epidemic was still mostly confined to China, officials there put huge cities on lockdown in order to stem the spread. Hundreds of flights into and out of the nation were canceled, and urban streets stood empty of cars. China’s burgeoning thirst for oil diminished, sending global crude prices into a downward spiral.
And when oil prices fall, it hurts states like New Mexico, which relies on oil and gas royalties and taxes for more than one-third of its general fund. “An unexpected drop in oil prices would send the state’s energy revenues into a tailspin,” New Mexico’s Legislative Finance Committee warned last August. Even the committee’s worst-case scenario, however, didn’t look this bad. Now, with COVID-19 spanning the globe, every sector of the economy is feeling the pain—with the exception, perhaps, of toilet paper manufacturers and bean farmers. But energy-dependent states and communities will be among the hardest hit.
At the end of December, the US benchmark price for a barrel of oil was $62. By mid-March, as folks worldwide stopped flying and driving, it had dipped to around $20, before falling into negative territory, and then leveling off around $10 in April. The drilling rigs—and the abundant jobs that once came with them—are disappearing; major oil companies are announcing deep cuts in drilling and capital expenditures for the rest of the year, and smaller, debt-saddled companies will be driven into the ground.
COVID-19 and related shocks to the economy are reverberating through the energy world in other ways. Shelter-in-place orders and the rise in people working from home have changed the way Americans consume electricity: Demand decreased nationwide by 10 percent in March. As airlines ground flights, demand for jet fuel wanes. And people just aren’t driving that much, despite falling gasoline prices, now that they have orders to stay home and few places to go to, anyway.
The slowdown will bring a few temporary benefits: The reduction in drilling will give landscapes and wildlife a rest and result in lower methane emissions. In Los Angeles, the ebb in traffic has already brought significantly cleaner air. And the continued decline in burning coal for electricity has reduced emissions of greenhouse gases and other pollutants.
But the long-term environmental implications may not be so rosy. In the wake of recession, governments typically try to jumpstart the economy with stimulus packages to corporations, economic incentives for oil companies, and regulatory rollbacks to spur consumption and production. The low interest rates and other fiscal policies that followed the last global financial crisis helped drive the energy boom of the decade that followed. And the Trump administration has not held back in its giveaways to industry. The Environmental Protection Agency is already using the outbreak as an excuse to ease environmental regulations and enforcement, and even with all the nation’s restrictions, the Interior Department continues to issue new oil and gas leases at rock-bottom prices.
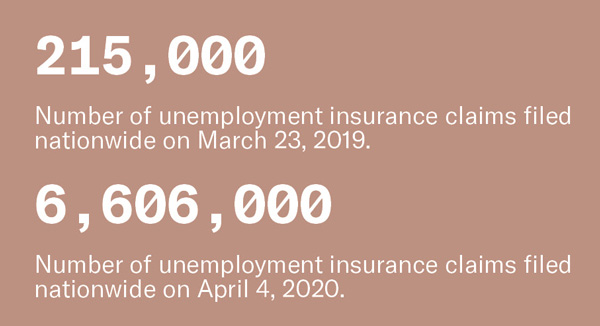
The impacts on energy state coffers will unfold over the coming weeks and months. But the shock to working folk from every economic sector has come swiftly. During the third week of March, more than 3 million Americans filed for unemployment—more than 10 times the claims from a year prior.
Infographic design by Luna Anna Archey. Sources: U.S. Energy Information Administration, New Mexico Legislative Finance Committee, U.S. Bureau of Labor Statistics, California Independent System Operator, Baker-Hughes, Unacast, FlightRadar24, Wyoming Department of Revenue, Carbon Footprint, International Air Transport Association, OAG.
Earlier this month, the New York City health department released a map showing confirmed COVID-19 cases by zip code. The highest case counts were concentrated in lower-income neighborhoods in Brooklyn, Queens, and the Bronx. The same week, the city released preliminary data highlighting higher rates of death among black and Latino New Yorkers.
Environmental advocates say that hazardous environmental conditions have contributed substantially to the coronavirus outbreak’s severity in New York City’s low-income communities of color.
The city’s data shows that a higher volume of cases are concentrated in neighborhoods with more environmental health hazards, according to Rachel Spector, director of the environmental justice program at New York Lawyers for the Public Interest, a nonprofit civil rights law firm. Major arterial highways, waste transfer facilities, power plants, and other polluting infrastructure create daily air quality challenges for residents of these neighborhoods—challenges that can take a cumulative toll on residents’ health, leading them to become more vulnerable in the face of a respiratory illness.
Three zip codes in Queens, for instance, have seen roughly 30 documented COVID-19 cases per thousand residents, which is double the citywide average. These neighborhoods—among them Astoria Heights, East Elmhurst, and Jackson Heights—are criss crossed by traffic-clogged highways like Interstate 278 and the Grand Central Parkway. Nearby sources of fine particulate matter—or PM 2.5, a pollutant particularly harmful to respiratory health—include LaGuardia Airport and several of the city’s power plants.
“It’s a classic environmental justice issue,” Spector told Grist. “You have a concentration of polluting infrastructure located in black and brown communities that are often high-poverty neighborhoods—people living in poor and crowded housing conditions, who continue to work and take public transportation because many of them are low-wage essential workers. So they’re disproportionately and continuously exposed.”
The coronavirus is not the only thing they’re exposed to, Spector added. Many of these communities disproportionately experience underlying health conditions as a result of years of chronic exposure to air pollution. The South Bronx, a predominantly low-income neighborhood of color, sees an annual average of 11 to 13 micrograms per cubic meter of fine particulate matter, compared to the World Health Organization’s air quality guideline of 10. The same area sees the city’s highest rate of emergency care visits for asthma as well as respiratory hospitalizations. It has also been among the neighborhoods hardest hit by COVID-19.
“The coronavirus is exposing the inequities that have been around for so long in our society,” Spector said.
The link between coronavirus deaths and pollution exposure is coming into focus. Earlier this month, Harvard researchers released a nationwide study that links long-term exposure to air pollution to increases in the exposed area’s COVID-19 death rate. They found that every additional microgram of PM 2.5 per cubic meter is associated with a 15 percent increase in the death rate from COVID-19.
Nevertheless, the EPA announced last week that it will not tighten or change the nation’s ambient air quality standards. Democratic lawmakers subsequently sent a letter to EPA Administrator Andrew Wheeler criticizing the decision. The senators cited evidence that air pollution in the form of fine particulate matter is detrimental to human health and could increase COVID-19 vulnerability, using New York City as an example.
Spector says that the areas hardest hit by the coronavirus—parts of Brooklyn, Queens, and the Bronx—also face acute challenges posed by particulate matter pollution. Although levels of PM 2.5 across the city aren’t as bad as those in areas near large-scale oil, gas, and chemical infrastructure, the EPA’s Environmental Justice Screening and mapping tool indicates that these New York City neighborhoods still have higher risks of cancer and respiratory illnesses from inhaling diesel emissions—conditions that could make them more vulnerable to severe COVID-19 complications.
Priya Mulgaonkar, a resiliency planner for the NYC Environmental Justice Alliance, co-wrote a 2016 report that analyzes the impact of truck traffic on the city’s air quality and the communities that host waste transfer facilities. One of the report’s key findings is that commercial waste trucks accounted for a significant amount of truck traffic, worsening the air quality of nearby communities, particularly in the South Bronx. These same communities ended up being among the hardest hit by COVID-19.
“The disparities for COVID-19 really mirror the disparities that New York City’s environmental justice communities have faced for decades,” Mulgaonkar told Grist. “Similarly to climate change, COVID-19 is really acting as a threat multiplier: exacerbating a lot of these inequalities that are due to environmental racism in New York City.”
Jelani Anderson formulated a plan before stopping to buy water at a convenience store in New Jersey. The 52-year-old Black man works as a safety professional and inspects construction sites all over the state. “I needed to make a stop to use the bathroom and get a water to maintain hydration,” Anderson told me in an email. “Given the difficulty in buying masks in this area, I only had a bandana to use as a nose and mouth covering.”
Anderson knew that the combination of racism and stereotyping means a Black man walking into a store with his face covered in a bandana could have an unfortunate outcome. He decided to keep on his reflective vest and work boots so he’d be easily identified as someone who, as he said, “belongs,” and to speak in a friendly tone to everyone near him. “This is not a time to startle an inattentive cashier or security guard by popping out of nowhere while being a Black man,” he explained. Anderson also decided to check his surroundings for any police officers and let a friend know he was about to make a stop.
The trip was uneventful; Anderson was able to take care of his business with no problems. But still, he was frustrated. “I was a bit angry by the extra tax I had to pay as a Black man,” he wrote, “devoting time and energy to not be overwhelmed by the anxiety of simply trying to protect myself and others from illness.”
It’s a feeling that is replicated across the country. The health effects from COVID-19 are disproportionately killing Black people. The United States has the highest rate of infection and death toll in the world. According to an investigation by my colleagues Edwin Rios and Sinduja Rangarajan, “In 20 of the 28 states plus DC for which a usable racial breakdown of infection data was provided, Black people make up a larger share of coronavirus infections than they do of the general population.”
They also face the additional threat of being seen as threatening when wearing a protective mask. “Some of the historical stereotypes about Blacks, particularly Black men, are related to criminality…strength and physicality, and these are stereotypes to supposedly be scared of,” Rashawn Ray, a sociologist at the University of Maryland, explained in a video for the Washington Post. When non-Black people who are unfamiliar with other races interact with Black people, those stereotypes can be at the forefront of their minds. “When they see Black men exhibiting a particular script, in this case, wearing a mask,” he noted, “what it signals to people is that they are trying to rob the store.” Ray said many Black people are making the same decisions as Anderson before going into essential businesses: “When Black men are getting ready to go out to a store to get essential goods for themselves and their families, they have to go through what I call a signaling process: ‘What are better ways that I can signal to people that I’m not a criminal?'”
In March, the Centers for Disease Control and Prevention advised that given the global shortage of personal protective equipment, masks should be reserved for health care workers. The agency also said that wearing a mask was unlikely to protect you from contracting the virus. Earlier this month, they reversed course and urged the public to cover their faces with some type of mask, including DIY cloth masks, when venturing out to the grocery store, to essential businesses, or public places. Some states are even requiring them in retail businesses, turning away anyone whose face isn’t covered up. An April 17 Gallup poll showed that 62 percent of Americans had worn masks in public in the last week.
For Black people, the familiar anxieties of simply existing in public intensified. Especially after a video from Wood River, Illinois, went viral. It depicted two Black men wearing masks being asked to leave a Walmart.
These fears and anxieties are not just anecdotal—they have some scientific research behind them. A 950-person experiment in 2017 by John Wilson, a psychologist at Montclair University, found consistent racial biases in participants. The group included multiple races and asked several questions related to race and perceptions. All of the respondents believed that Black men were larger and more powerful than same-sized white men. They also believed that the Black men were more likely to cause harm in an altercation and that police would be justified in using force against them. Black respondents also believed Black men were stronger and larger, but they did not believe they were capable of causing more harm or were deserving of more police force. Wilson concluded that these findings could explain why Black men are more likely than white men to be shot and killed by police, explaining “this research suggests that misperceptions of black men’s size might be one contributor to police decisions to shoot.”
A 2019 Washington Post study showed that Black people were disproportionately killed by police compared to white people, between the years 2015 and 2019. In addition, they found that Black men are more likely to be fatally shot while unarmed. So, it’s no surprise that Anderson, Young, and other Black men are weary of making themselves even more of a target for biased police officers.
The names of Black people shot and killed for doing everyday activities seems endless. In 2014, 17-year-old Jordan Davis was shot and killed in his car by a white man who didn’t like that he was playing his music loudly. In 2018, 26-year-old Botham Jean was killed inside his own apartment when white police officer Amber Guyger, mistaking his home for her own, shot and killed him. And last year 28-year-old Atatiana Jefferson was shot and killed through the back window of her home by Aaron Dean, a white police officer who was responding to a call from a neighbor who said Jefferson’s front door was open.
But it’s not just the men who worry. Black women also have experienced racial profiling and violence just for existing in public while being Black. “My mind instantly went to Sandra Bland,” Alaia Williams, a 35-year-old Black woman who works as a business operations strategistin the Los Angeles area told me, referring to the woman in Texas who died in jail after getting stopped and arrested in 2015. The thought of getting pulled over by police for no reason and having that action escalating into tragedy crossed Williams’ mind plenty of times in the past. Now, the thought of driving with her face covered has added to her anxiety. “If you’re Black doing anything, you can be profiled,” she said. “There’s this anxiety that comes with it, regardless of your gender.”
For many Black people, weighing whether or not to wear a mask comes down to deciding whether or not to risk getting racially profiled, which could turn deadly, or contracting COVID-19, which could also turn deadly. “Am I going to risk my health or am I going to risk it all and pray that no one in this open-carry state mistakes me for a volatile?” George Wesley, a Black man from Newport News, Virginia, told me. The 32-year-old freelance video editor and graphic designer alters his behavior depending on his surroundings. At a grocery store with diverse patrons, he feels comfortable wearing his mask. But if the store is mostly white, he tries a different approach. “I will take my mask down to make them feel comfortable, compromising my health,” he says. “Black with a mask is a gamble.”
Some intrepid reporters at the Washington Post have waded through transcripts of all 35 White House coronavirus press briefings since March 16 and analyzed more than a day’s worth of President Donald Trump’s statements. What they found isn’t pretty, but it isn’t surprising.
Philip Bump and Ashley Barker, who looked closely at Trump’s remarks from April 6 to April 24, write that his “freewheeling approach” to his daily briefings closely resembles his on-pause campaign rallies. In nearly a quarter of his prepared statements and answers to reporters’ questions, Trump said something false or misleading, such as suggesting that injecting household disinfectants into the body might cure COVID-19. (Please don’t do this.)
In their review of 13 hours of Trump remarks over the last three weeks, Bump and Barker found:
45 minutes of self-praise
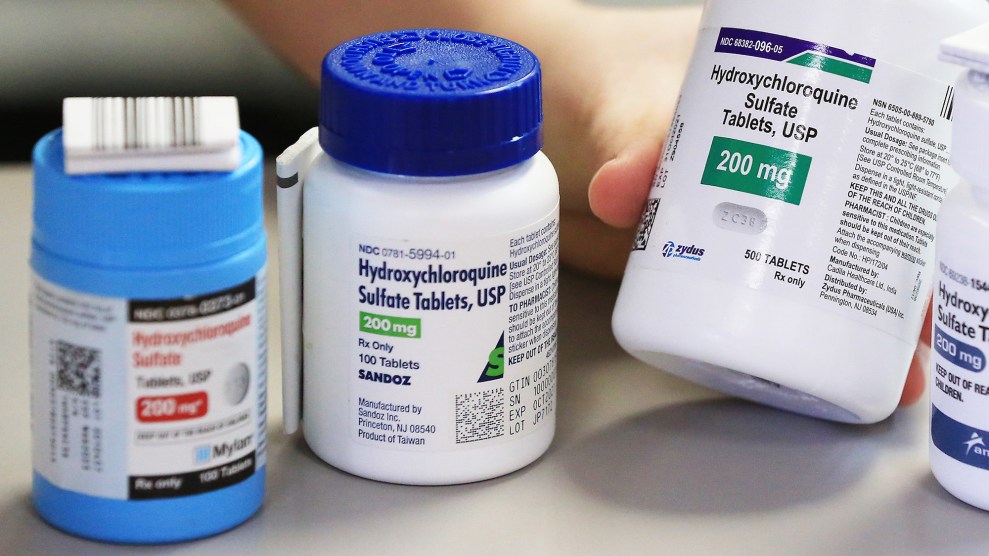
9 minutes promoting hydroxychloroquine, an anti-malarial drug that the FDA issued a warning about on Friday, saying it should not be used outside a hospital setting
4 and half minutes of condolences for COVID-19 victims
Altogether, Trump has spoken for more than 28 hours since he started his daily briefings in March. In comparison, we’ve heard from Dr. Deborah Birx, the White House coronavirus response coordinator, for 6 hours cumulatively, and Dr. Anthony Fauci, the country’s top infectious disease expert, for just 2.
Of his answers to 346 questions that Trump has been asked, he has responded by attacking someone in a third of his answers. The most common targets of those attacks were:
Democrats, including Barack Obama and Nancy Pelosi (attacked 48 times over 30 minutes)
The media (attacked 37 times over 25 minutes)
Governors (attacked 34 times over 22 minutes)
China (attacked 31 times over 21 minutes)
In some alternate universe, it might have been reassuring, or at the very least informative, for the president of the United States to spend such a significant chunk of time speaking to the public during a global crisis that has killed more than 50,000 Americans and cratered the economy. But who are we kidding? At least the president’s “ratings” were “through the roof”:
I’ve had great “ratings” my whole life, there’s nothing unusual about that for me. The White House News Conference ratings are “through the roof”(Monday Night Football, Bachelor Finale , @nytimes) but I don’t care about that. I care about going around the Fake News to the PEOPLE!
At a White House briefing room and in a radio interview last week, Vice President Mike Pence pushed the message that the coronavirus epidemic would be mostly over by “early summer.”
“If we continue these mitigation efforts in the days ahead, as states implement their policies—including phased reopening that will preserve those gains—we do believe by early summer we could be in a much better place as a nation, with much of this coronavirus epidemic behind us,” Pence said Thursday at the president’s daily coronavirus briefing.
But that doesn’t mean social distancing is going away anytime soon, even though some states have already decided to begin reopening. On Sunday, White House coronavirus response coordinator Dr. Deborah Birx said that social distancing guidelines will continue through the summer.
On NBC’s “Meet the Press” Sunday morning, Birx was asked about a statement by Pence Friday that by Memorial Day, COVID-19 would be “largely…behind us.” “This Memorial Day? 2020? Is that realistic?” host Chuck Todd asked.
In response, Birx said that data from Louisiana and Detroit, where COVID-19 cases may have already peaked, “gives us great hope” for hard-hit areas like New York City, possibly explaining the vice president’s comments. But, she added, “social distancing will be with us through the summer, to really ensure that we protect one another.”
TODAY: Vice President Mike Pence said COVID-19 will be largely “behind us” by Memorial Day.
Dr. Birx: “Social distancing will be with us through the summer to really ensure that we protect one another.” pic.twitter.com/ksYFZJFUNL
It’s not clear whether Birx’s comments will mean all that much. Just over a week ago, Trump was screaming on Twitter to “LIBERATE” states from public health orders. With nail salons and barber shops already open in Georgia and Oklahoma, and Colorado, Minnesota, and Montana planning to ease up on restrictions this week, the White House has so far allowed governors to choose when and how to lift social distancing guidelines.
As Americans continued to roll their eyes at his comments about injecting disinfectant to kill the coronavirus, President Donald Trump mainlined a fresh dose of misinformation and grievance into his Twitter stream yesterday.
First, he continued to try to relitigate his widely mocked press briefing on last Thursday, claiming his widely mocked suggestions were not directed at Dr. Deborah Birx, the response coordinator for the White House Coronavirus Task Force, but William Bryan, the Department of Homeland Security undersecretary for science and technology.
Was just informed that the Fake News from the Thursday White House Press Conference had me speaking & asking questions of Dr. Deborah Birx. Wrong, I was speaking to our Laboratory expert, not Deborah, about sunlight etc. & the CoronaVirus. The Lamestream Media is corrupt & sick!
Trump did ask Bryan whether UV light could be used to “hit the body” or somehow used “inside the body, which you can do either through the skin or in some other way.” But he also addressed Birx directly when he said, “I would like you to speak to the medical doctors to see if there’s any way that you can apply light and heat to cure…Deborah, have you ever heard of that? The heat and the light, relative to certain viruses, yes, but relative to this virus?”
Next, Trump suggested that he’d soured on press briefings because the media “refuses to report the truth of facts accurately.” (By the way, the quotes in the previous paragraph are verbatim from the White House website.) Nearly a month ago, he’d bragged that his daily briefings had made him “a ratings hit.” Now Republicans are worried that his briefings are hurting them politically; one senator told the New York Times “the nightly sessions were so painful he could not bear watching any longer.”
What is the purpose of having White House News Conferences when the Lamestream Media asks nothing but hostile questions, & then refuses to report the truth or facts accurately. They get record ratings, & the American people get nothing but Fake News. Not worth the time & effort!
The president, who spent weeks pushing an untested malaria drug as a COVID-19 treatment, then prescribed a dose of “common sense.” (On April 5, he’d touted hydroxychloroquine yet again, saying “What do I know? I’m not a doctor. I’m not a doctor. But I have common sense.”)
Remember, the Cure can’t be worse than the problem itself. Be careful, be safe, use common sense!
Finally, Trump claimed that the Democrats and media have falsely accused him of calling the coronavirus pandemic “a Hoax.”
I never said the pandemic was a Hoax! Who would say such a thing? I said that the Do Nothing Democrats, together with their Mainstream Media partners, are the Hoax. They have been called out & embarrassed on this, even admitting they were wrong, but continue to spread the lie!
Let’s look at the transcript from the president’s rally in North Charleston, South Carolina, on February 28 (italics mine):
So far we have lost nobody to coronavirus in the United States. Nobody. And it doesn’t mean we won’t and we are totally prepared. It doesn’t mean we won’t. But think of it, you hear 35 and 40,000 people [dying from flu] and we’ve lost nobody. You wonder if the press is in hysteria mode… Now the Democrats are politicizing the coronavirus. You know that, right? Coronavirus. They’re politicizing it… And this is their new hoax. But you know we did something that’s been pretty amazing. We have 15 people in this massive country and because of the fact that we went early, we went early, we could have had a lot more than that.
If you read that and conclude the president was minimizing the seriousness of an impending public health crisis by accusing the media and Democrats of exaggerating its dangers, perhaps you don’t recognize sarcasm.
Utah residents may be lukewarm on President Donald Trump—the president leads Democrat Joe Biden there by only five points, a shocking number in such a reliably red state—but Utah has proven to be an enthusiastic booster of Trump’s favorite coronavirus miracle cure, the anti-malaria drug hydroxychloroquine. On March 21, a group of drug promoters in the state held a press conference to advocate for its use to treat Covid-19, claiming it could practically raise the dead, despite the fact that there’s no evidence that it works, and plenty of evidence that it can be dangerous to some people.
“There are responses that are equivalent to Lazarus—literally the biblical Lazarus—people almost dead coming back,” physician Kurt Hegmann, director of the Rocky Mountain Center for Occupational and Environmental Health at the University of Utah, said at the event.
Ten days later, the state spent $800,000 to purchase 20,000 doses from a local pharmacy chain, Meds in Motion, whose owner had been promoting the drug to state officials for weeks. The state legislature planned to set aside $8 million to buy 200,000 more doses to distribute free of charge to anyone diagnosed with COVID-19. Experts warned that the purchase was a waste of money given that the drug hasn’t been proven to work in treating the disease.
Eight million dollars for pharmaceuticals is a lot of money in a state that ranks dead last in per-pupil public school spending and spent most of the last decade refusing to expand Medicaid under Obamacare, even after state residents passed a ballot initiative demanding the expansion.
Utah House Democrats were suspicious of the GOP state officials’ enthusiasm for the unproven drug. They released a press statement criticizing the purchase, noting that their GOP colleagues had been pushing to buy the drugs from Dan Richards, the owner of Meds in Motion, who had amassed huge quantities of the raw materials needed to compound the drug and now wanted the state to buy his stash. Citing a recent study showing that hydroxychloroquine may endanger coronavirus patients, the state democrats said on April 21, “[O]ur colleagues quietly pushed the state to buy the stockpile of Dan Richards of Meds In Motion, a pharmacist lobbyist, with precious taxpayer dollars to compound the unproven drug without public scrutiny.”
“There is absolutely no need for us to spend money on this drug now,” they added. “It is also not clear how the decision to use state money was made, or where the money is coming from.”
Nonetheless, Utah officials moved forward, urged on by state Senate President Stuart Adams, who had appeared at the March press conference with Richards and the other drug promoters. But on Friday, after the FDA warned against negative impacts of the drug, Governor Gary Herbert announced that the state would not purchase any more hydroxychloroquine. He claimed to have no idea how the first batch got procured by his administration, which issued the no-bid contract under emergency procurement rules enacted because of the pandemic.
The 20,000 pills haven’t yet been delivered to the state health department, so Herbert suggested that the state should get a refund. “That’d be nice if they just said, you know, we had a miscommunication here and we’re apologizing and here’s your money back,” he said at a news conference Friday.
Can you pitch in a few bucks to help fund Mother Jones' investigative journalism? We're a nonprofit (so it's tax-deductible), and reader support makes up about two-thirds of our budget.
We noticed you have an ad blocker on. Can you pitch in a few bucks to help fund Mother Jones' investigative journalism?
This is where you come in.
We’re a nonprofit newsroom, because the truth-telling investigations we do don’t happen under corporate ownership. We get to shine a bright light into the dark corners of power and report stories other media are afraid to touch.
The essential ingredient that makes this possible? Readers like you.
We’ve got a lot of hard, consequential work to do in the weeks and months ahead, and we can’t do it without reader support. Please stand up for independent media and make a donation today.
This is where you come in.
We’re a nonprofit newsroom, because the truth-telling investigations we do don’t happen under corporate ownership. We get to shine a bright light into the dark corners of power and report stories other media are afraid to touch.
The essential ingredient that makes this possible? Readers like you.
We’ve got a lot of hard, consequential work to do in the weeks and months ahead, and we can’t do it without reader support. Please stand up for independent media and make a donation today.









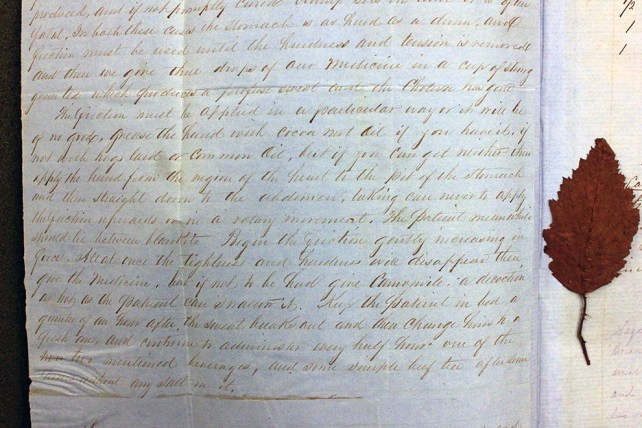
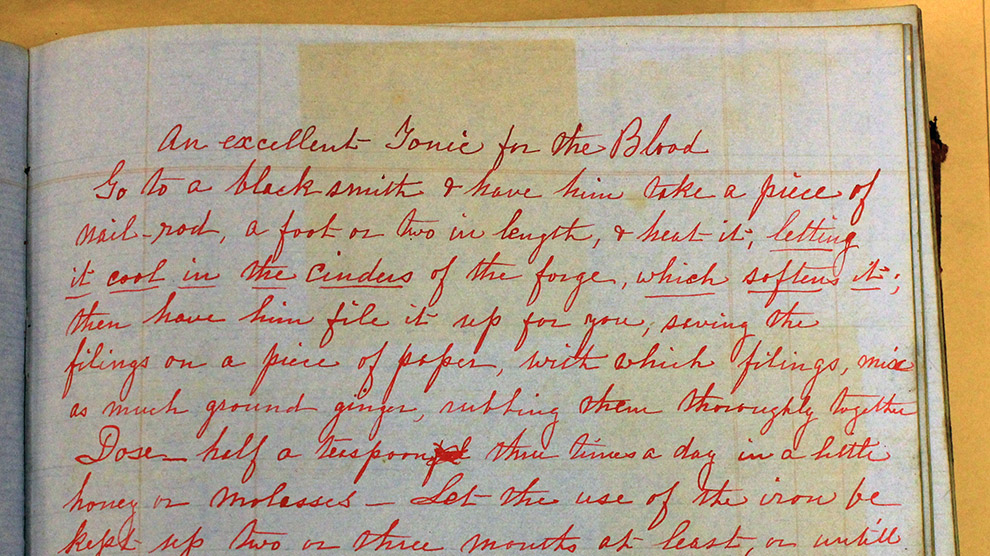




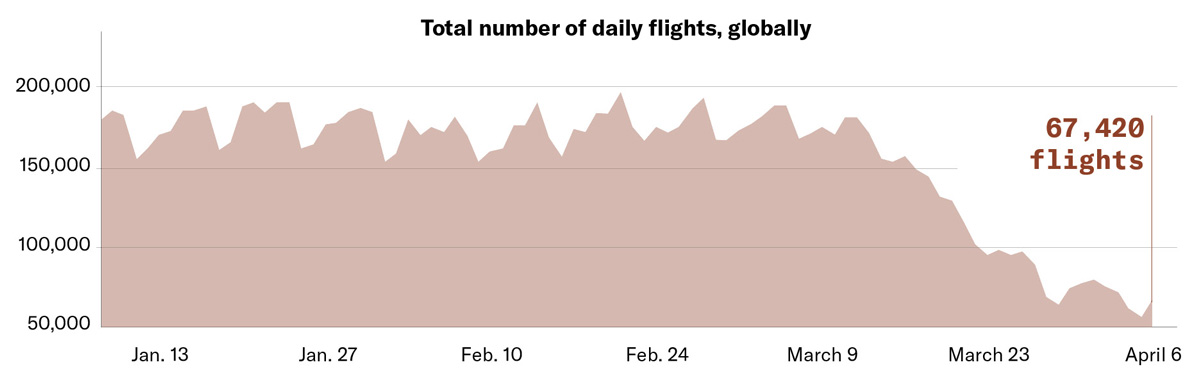
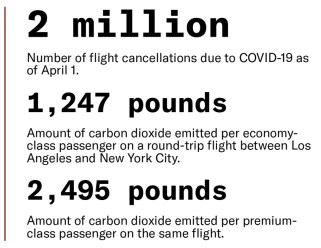
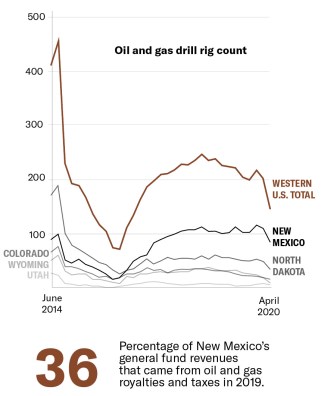
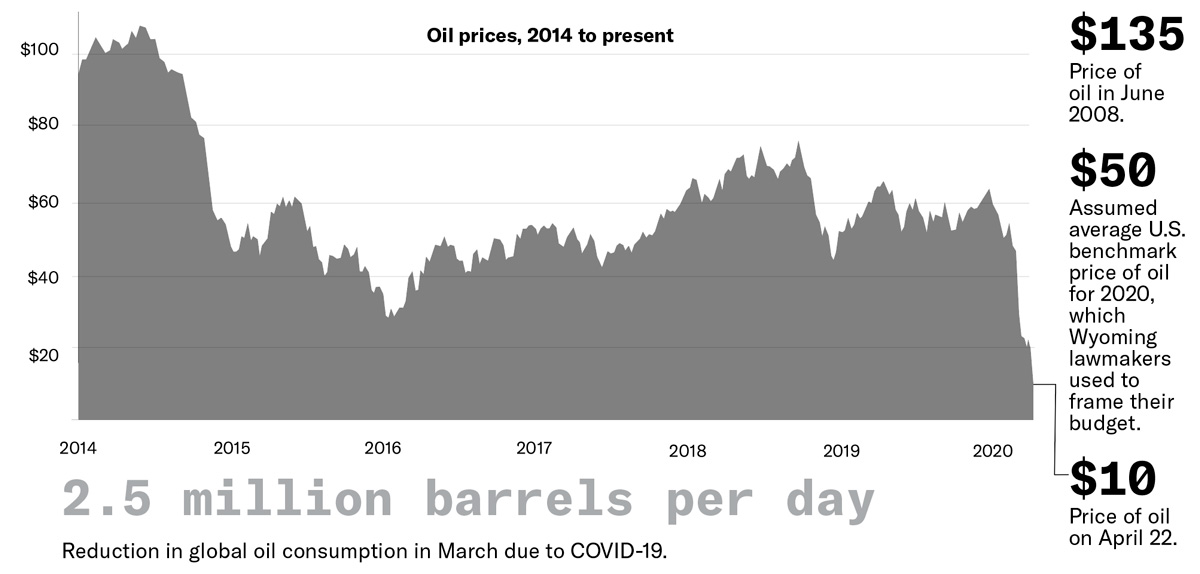
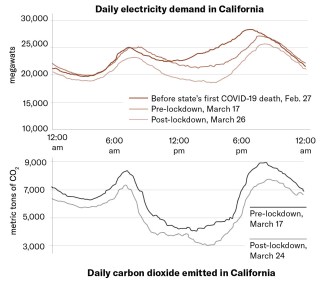
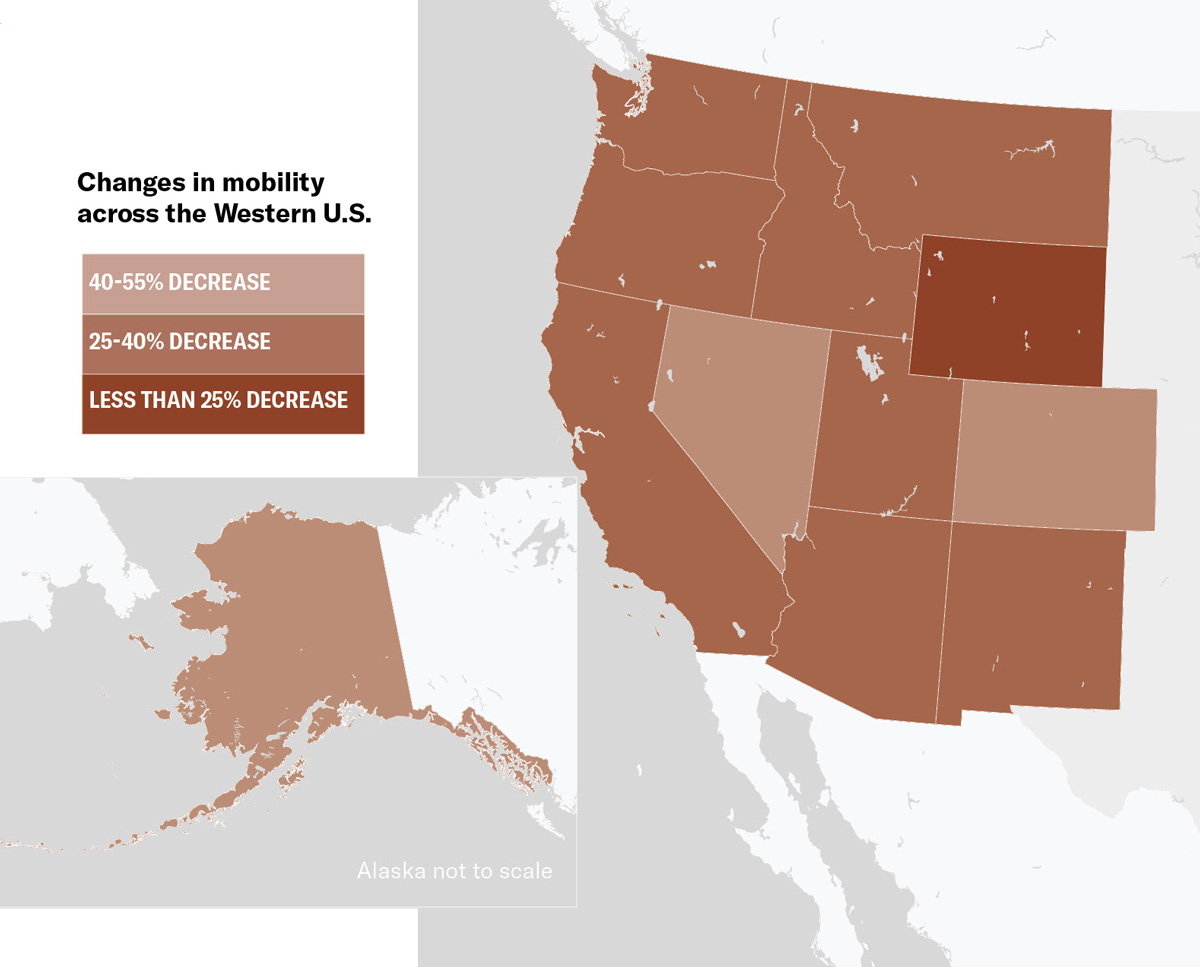 The slowdown will bring a few temporary benefits: The reduction in drilling will give landscapes and wildlife a rest and result in lower methane emissions. In Los Angeles, the ebb in traffic has already brought significantly cleaner air. And the continued decline in burning coal for electricity has reduced emissions of greenhouse gases and other pollutants.
The slowdown will bring a few temporary benefits: The reduction in drilling will give landscapes and wildlife a rest and result in lower methane emissions. In Los Angeles, the ebb in traffic has already brought significantly cleaner air. And the continued decline in burning coal for electricity has reduced emissions of greenhouse gases and other pollutants.