RESPONSE TO JENNIFER GONNERMAN’S ARTICLE, “SCHOOL OF SHOCK”
Matthew Israel
Response
Every surgical, dental or medical treatment involves discomfort, risks or costs on the one hand, and expected benefits on the other. For most persons a reasonable approach is to weigh the discomfort/risks/costs against the potential benefits in deciding whether to undergo or approve the treatment. In the case of certain treatments, however, there are some persons who, for religious or philosophical reasons, are unwilling to weigh the negative aspects of those treatments against the potential benefits. These persons view the treatment in question as Wrong with a capital “W,” regardless of the potential benefits the treatment might produce. For example, Christian Scientists oppose the use of medical interventions, and Scientologists oppose the use of psychiatric drugs, regardless of what potential benefits may ensue.
Opponents of behavior modification treatment that involves aversives (sometimes referred to as “aversive therapy”) are similarly unwilling to weigh the discomfort, risks or costs associated with aversives against the potential benefits—even when those benefits could be lifesaving, life-improving or life-extending. Such persons prefer to brand aversives as “Wrong,” refusing to recognize them as part of a relatively new behavior modification treatment procedure2, and many of them sometimes do whatever they can to prevent anyone else from using them. It is clear from Ms. Gonnerman’s article that she is one of those persons.
Ms. Gonnerman is so intent on indicting the Judge Rotenberg Center (“JRC”), the only special needs school in the country that offers this form of therapy, that she violates the normal journalistic ethics of presenting both sides of a controversial issue. Out of a total of 265 column inches that her article occupies, only 15 inches (six percent of the article) presents any of the benefits of JRC’s treatment. Even those few accounts of parents (characterized as “desperate parents”) or students who speak positively about JRC are presented with snide comments, disparaged by unfavorable observations or reported in the least favorable light possible. For a more accurate picture of JRC, the reader is encouraged to consult http://www.judgerc.org/introtojrc.html. Ms. Gonnerman grossly misrepresents JRC’s treatment. The treatment is overwhelmingly based on an innovative, unique and comprehensive system of rewards and behaviorally-designed educational procedures that feature self-instructional software that each student accesses through his or her own computer. The treatment eliminates or minimizes the use of psychotropic drugs—a form of treatment that is far more dangerous and intrusive than anything done at JRC.
Aversives, in the form of a brief, two-second skin shock to the surface of, typically, the arm or leg, are added to this treatment for only certain extremely difficult-to-treat behaviors of that have failed to respond to positive-only treatment in the student’s previous placements as well as at JRC. The procedure feels like a hard pinch and, unlike the heavy and often ineffective psychotropic drugging that this procedure typically replaces, has no negative side effects. Rewards and educational procedures alone are tried for an average of 11 months at JRC before JRC considers the addition of aversives. In addition, the use of aversives has to be pre-approved, on an individual basis, by the child’s school system (through the IEP process), the parent, a physician, a psychiatrist, a human rights committee, a peer review committee and a Massachusetts Probate Court judge.
Currently, only a minority of JRC’s school-age students receive skin shock as an aversive and even in these cases its use is very infrequent, less than once per week in the average case. In many cases the student progresses so well with this treatment that the aversives can eventually be removed entirely and the student can be returned to his/her local school system.
Ms. Gonnerman devotes extensive space at the very beginning of her article to the stories of two students whose parents became dissatisfied with JRC and withdrew their students (a routine event in every residential school). No comparable space is given to the hundreds of students whose parents are thrilled with the changes in their children that JRC was able to accomplish and that no previous program was able to achieve. Ms. Gonnerman also devotes space to the fact that during JRC’s 35-year history, a few students have died from natural causes that had nothing to do with the treatment they received at JRC. The only apparent purpose of this inclusion is to cast negative aspersions on JRC that have no basis in fact. The reader is not told that JRC has a unique no-rejection, no-expulsion policy that means it accepts students who have pre-existing, life-shortening medical conditions.
Ms. Gonnerman reports on the views of a few psychologists who are opposed to JRC’s treatment. No space is given to the many psychologists who admire JRC’s work and who wish their own agency had the ability to provide the treatment procedures that JRC is able to offer. Ms. Gonnerman publishes anonymous critical comments made by some former employees of JRC, eight of whom she interviewed. One of these was probably Greg Miller, a disgruntled former employee who appeared with Ms. Gonnerman on National Public Radio , a piece that was stimulated by her article. Mr. Miller worked enthusiastically for JRC for three years during which he failed to raise any objections to JRC’s treatment to anyone. If he had seen anything abusive and failed to report it while employed at JRC, he violated his duty to report any suspected abuse to the appropriate state agency. After three years of employment, he was disciplined for insubordinate actions and then promptly resigned. No space is given to the hundreds or thousands of current or former staff members who have positive things to say about JRC.
The reader is not told that JRC is the only program in the country that is able to offer effective, lifesaving treatment to students with severe self-abuse and aggression or that other programs that try to serve such students, but which are unable to serve them successfully, often expel those students and refer them to JRC for successful treatment (see here).
Ms. Gonnerman objects to JRC’s use of aversive therapy to treat the self-destructive or aggressive behaviors of “higher functioning” special needs students who have the ability to speak and interact normally. Yet these students are often the most eloquent defenders of this therapy; many credit it with saving their lives or turning their lives around in a positive direction. Why prevent such youngsters from benefiting from this therapy just because they have relatively normal cognitive functioning? Normal adults can obtain aversive therapy from a psychologist to treat behavior problems such as excessive smoking, gambling or eating. Why should special needs students with normal cognitive functioning be unable to obtain aversive therapy for their particular behavior problems?
Ms. Gonnerman quotes from an inaccurate report by the New York State Education Department, but does not tell the reader that it was prepared as part of a campaign to deny New York students the possibility of benefiting from aversive therapy—a campaign that is currently being challenged in federal court by 50 JRC parents from New York State. She also fails to note that three Massachusetts agencies have investigated JRC and found no support for the major findings of that report. Ms. Gonnerman objects to the fact that effective behavioral treatment requires aggressive treatment of the earliest recognizable stages of problematic behaviors and of the behaviors that typically precede problem behaviors (“antecedents”) even though those behaviors may, if viewed out of context, appear to be benign. This practice is comparable to the need to provide early detection and treatment for cancer and other serious diseases. The early forms of such diseases may look benign, but if left untreated can grow into life-threatening forms. The same is true of certain seriously problematic behaviors.
And, most important, Ms. Gonnerman fails to put the risks/intrusiveness of aversive therapy with skin-shock into proper perspective. Behavioral treatment with skin shock at JRC involves a brief, two-second period of discomfort that has no significant side effects. It is a procedure which, when combined with a program that is overwhelmingly based on rewards and educational procedures, enables JRC to take students off of all psychotropic medication, give them an education for the first time in their lives, and give them and their parents hope and optimism for their future where none had previously existed.
Without aversive therapy, the alternatives, for many of the students who are referred to JRC, are being heavily drugged with life-shortening and medically dangerous psychotropic medications,3 being warehoused in institutions or jails without receiving any treatment at all, being confined and/or frequently restrained in padded isolation rooms, bouncing in and out of psychiatric hospitals with no improvement, killing or maiming themselves or others with their own self-abusive behaviors or aggressive behaviors, or simply ending up homeless on the streets.
More Detailed Response
Jennifer Gonnerman’s article “School of Shock” (Mother Jones, September/October 2007) is a biased and misleading account of the Judge Rotenberg Center (“JRC”) that is best characterized as a hatchet job. Ms. Gonnerman persuaded JRC and the Parents of the JRC students to allow her to come to JRC and observe the school and the students by very cleverly and falsely pretending to be sympathetic to the cause of the JRC students and their parents. She asserted that she had read all the letters from the parents on the JRC web site and had cried while reading them. In addition, she represented that the article she was writing would be published in the New York Times Sunday Magazine, a magazine that has a reputation for printing serious, balanced, non-sensational articles. The Times even flew a very artistic photographer and assistant from San Francisco to do the photography. After the article was written it did not appear in the Times. When we asked Ms. Gonnerman why, she said the Times had rejected it because it was not of sufficiently national interest.
Now that we have seen the article, it seems more likely that the Times rejected the article as a biased, unfair and misleading hatchet job. Ms. Gonnerman has shamefully exploited the severely disabled JRC students and their parents. She ignores or glosses over JRC’s treatment successes, all the evidence that supports the use of aversives, and the plight of its students before attending JRC. The many court victories won by the JRC parents to preserve the JRC treatment program are a matter of public record and should have been investigated by Mother Jones before the magazine printed Ms. Gonnerman’s fallacious article.
This type of a dishonest article could have been written about any topic, no matter how benign. Ms. Gonnerman could have written such a negative article about freshman life at any university, for instance. She could write about the cramped and cluttered conditions of the dormitory, the terrible food, the homesickness, the late nights with little sleep, the incredible long lines at the registrar’s office and the bookstore, the overcrowded classrooms, the high tuition, and the exposure to underage drinking. She could also add lies to further sensationalize her story, as she did with the JRC article, by reporting that most students cry themselves to sleep because they are so depressed and many are dangerously gaunt due to the bad food. Ms Gonnerman could make college sound like a horrible, abusive place by not mentioning all the positive aspects of college life—for example, all of the interesting subjects the students learn about, the exposure to talented and fascinating professors and other lecturers, exposure to the arts, learning how to do research and write on a college level, learning about and choosing a career, meeting and getting to know fellow students from around the world, meeting the people who will be friends for life, and learning how to live independently from their parents.
This distorted report of college life is similar to the distorted report of JRC that Ms. Gonnerman created. A fraudulent article about college life is not as harmful as a distorted report on JRC, however, because many people have attended college and will know right away that the article is dishonest. What makes Ms. Gonnerman’s article so harmful and exploitive is the fact that only a tiny fraction of the population has had any exposure to severe behavior disorders. In order to understand JRC in its proper context, the following points must be made, none of which were explained in Ms. Gonnerman’s article.
- It is well documented in scientific articles and in court findings that some special needs children and adolescents have behaviors that are so self-abusive, aggressive or destructive as to be life-threatening and self-maiming. Consider, for example, just one type of behavior—self-abuse. Some special needs children referred to JRC have shown self-abusive behaviors such as banging their head to the point of brain damage, biting off their own fingertips, pulling out their teeth, vomiting and refusing food to the point of starvation, biting a hole through their cheek, biting off part of their own tongue, scratching their heel to the point of blood, bone infection and eventual death, breaking their own arm, cutting off their own earlobe with a scissor, running into moving traffic, punching their eyes causing detached retinas and blindness, pulling out their hair to the point of baldness, swallowing X-Acto knives, and cutting their skin with a knife so often that the skin becomes too tough to suture.
- Children with such very severe problem behaviors usually cannot be successfully educated in public schools. When a public school encounters such a student, the school will refer the student to a psychiatric hospital or to a nonpublic, special needs school where the student is often not effectively treated. Instead, the student is usually drugged into a stupor. If students are given high enough dosages of psychotropic drugs, these drugs will sedate them so much that the students are incapable of hurting themselves or anyone else—but such students are also incapable of participating in education or even communicating with their family. These drugs also have many debilitating side-effects including kidney damage, liver damage, tremors, obesity, and lock jaw and many effects are permanent. Unfortunately many so-called experts in this field will refer to this drug stupefaction as a treatment success.
Other so-called effective treatments for severe behavior disorders that JRC has seen in the histories of newly admitted students include lobotomy, removal of teeth (for severe biters), constant seclusion, constant mechanical restraint, and many others that experts refer to as “more humane and effective” alternatives to JRC’s aversive therapy procedures. The lack of effective alternatives and the sheer cruelty of drugging a child into a near coma is why parents turn to a non-public, special needs school such as the Judge Rotenberg Educational Center that is specially equipped to manage and educate the student, and has a proven track record of saving students from the ravages of constant heavy sedation. A real journalist would have mentioned these facts and, more importantly, investigated why the anti-aversive experts are hiding the fact that there are no effective treatment alternatives for severe behavior disorders. A real journalist would have asked why the JRC students have, prior to coming to JRC, spent so many wasted months or years sedated in a psychiatric ward and why their parents had to fight to get their child out of a psychiatric ward and into a special needs school such as JRC. Finally, a real journalist would have investigated why schools and clinicians fear being blackballed if they use, or admit to using aversives. As a result of this fear, children are forced to suffer with untreated painful behavior disorders, to receive no education and to have no social life of any kind.
- Most nonpublic, special needs schools that try to educate and treat such students use rewards, education and positive-only procedures. Unfortunately, studies show that positive-only treatment procedures are effective in only 6o percent of the cases at most and cannot handle the most severe behavior problems.
- Actually, although most nonpublic, special needs schools pride themselves on using “positive-only” treatment procedures, the truth is that such programs really do use aversives without calling them by that name. In other words, such schools use hidden aversives such as these:
- Five to eight staff members wrestle the student to the floor, each time he/she is aggressive, and hold him/her there until he/she stops struggling. The procedure could last an hour or more. This is a procedure that JRC is able to eliminate entirely whenever it is able to use effective aversives such as the two-second skin-shock procedure.
- If a student is aggressive, staff members may grab the student and take him/her, against his/her will, into a “time-out” isolation room and leave him/her there for a specified period of time. This is a procedure that JRC never uses.
- Staff members may hold the student tightly (manual restraint) each time he/she is aggressive and thereby prevent the student from doing anything at all.
- Staff members may grab the student forcefully by the shoulder or arm and squeeze hard while giving the student a so-called “physical prompt” to engage in a certain action.
- Staff members may force the student to engage in some physical action against the student’s will over and over. This is called “overcorrection” or “positive practice” but it will only work to decelerate a behavior if it done in a manner that is aversive.
- JRC does not use hidden aversives such as these preferring, instead, the more honest course of using fully-disclosed and more effective aversives such as skin-shock.
- The typical nonpublic, special needs school will, in addition to the use of such hidden aversives, have a psychiatrist prescribe large quantities and a wide variety of psychotropic drugs to students with severe behavior problems. If a student is given enough drugs, he or she will essentially be put into a drug-induced stupor for much or all of the day. Such medication can be so drugging that the student may not be able to recognize his own parents and might fall face-first into his food at mealtime. Unfortunately, for some students even large quantities of drugs are insufficient to control their aggressive or self-abusive behaviors. By contrast, JRC’s policy is to avoid totally, or at least minimize, the use of psychotropic medication.
- For some students the typical nonpublic special needs school may find that if the school places no educational or behavioral demands on the student, the student will refrain from aggression, self-abuse or destructive behaviors. If this is the case, such a school may choose to solve the problem by essentially “warehousing” the student—i.e., keeping the student safe and adequately fed, but not undertaking any serious attempt to educate the student or change the student’s behaviors.
- In extreme circumstances, the typical nonpublic, special needs school might do things such as call in the police to handcuff the student when he or she is aggressive, or send the student to a psychiatric hospital. JRC never calls in the police to deal with aggressive or otherwise disruptive students and JRC is an effective alternative to psychiatric hospitals.
- In the case of certain students with case-hardened problem behaviors, the school may try all of the above procedures—positive-only procedures, hidden aversives, seclusion, restraint, drugs, warehousing, calling in the police and sending the student to a psychiatric hospital—and may find that none of them are successful in controlling the student’s problem behavior. In addition, the school may at some point simply tire of seeing the student continually harm the school’s staff members, other students, and property. At that point many such schools will expel the student. Sometimes, however, some students are aggressive even to their own parents. Consequently, at that point the parents, may even be unable or afraid to allow the students to come home. This leaves the parent with essentially no options. Such students are then left to live in the street, to languish in homeless shelters, to bounce in and out of psychiatric hospitals again or to commit some offense and be jailed. These students, i.e., those who are expelled from such schools that use positive-only treatment procedures, are the ones that are referred to JRC, where they finally can receive effective treatment.
- Before JRC uses aversives with any student, only positive and educative procedures are employed for an average of 11 months to try to change serious problematic behaviors. The positive procedures that JRC employs include many rewarding and educational procedures. The extent and variety of the reward systems at JRC will not be found at any other program. They include the following:
- an all school arcade-type reward lounge
- a retail store in which students can purchase desired items for themselves or others
- a reward corner in many of the classrooms in which the student can relax, watch tv, play games, etc.
- a reward box in many classrooms containing items that students can earn through their behaviors
- a reward afternoon once per week that features a barbecue and games; (6) frequent field trips used as rewards
- electronic game devices in each bedroom
- opportunities to order food out from local restaurants
- internet usage
- a student discussion board
- various sports activities, etc.
- JRC’s positive and educational procedures alone are currently effective with about half of its school-age students. For the other half, however, positive and educational procedures need to be supplemented with the use of a brief aversive. The most effective aversive available is a two-second, harmless shock to the surface of the skin, typically of the arm or leg. It is extremely effective. For example, in treating aggression, we are able to accomplish a 95 percent reduction in 96 percent of the cases, within a matter of weeks. As a result, students can begin to receive an education and benefit from positive programming for the first time in their lives. Unlike drugs, the treatment has no significant side effects and the treatment can be discontinued for many students as their behavior improves. Parents and students describe the improvement as life-saving.
- There are many safeguards at JRC to make sure that the skin-shock procedure is used carefully, professionally and properly. They include prior parental consent, prior individualized court authorization (the judge appoints an attorney to represent the child’s interests in this process), prior approval by a Human Rights Committee and a Peer Review Committee, clearance from a physician and a psychiatrist to insure that there are no medical contraindications, etc. More information about these safeguards may be found on JRC’s website.
- Only a minority (43 percent) of JRC’s school-age students are currently receiving skin shock treatment. And for those who are being treated with skin-shock, the average student receives only one application per week. More information about the frequency with which skin-shock is used at JRC may be found on JRC’s website.
- To summarize:
- JRC treats severe problem behaviors of special needs children and adults who have failed in every other program that has been tried with them.
- Programs that use “positive-only” treatment procedures expel students with really severe behavior problems and these students are often then referred to JRC.
- JRC removes students from psychotropic drugs and applies a highly consistent behavioral program of positive rewards and educational procedures for an average of 11 months before considering the use of any aversive.
- If rewards and educational procedures alone prove to be insufficiently effective, they are supplemented, when necessary, with a two-second shock to the surface of the skin, used as a corrective consequence for the problem behavior.
- Before employing skin-shock, JRC obtains consent from the child’s parent and individualized approval from a probate court judge, a physician, a psychiatrist, a peer review committee and a human rights committee.
- JRC’s skin-shock procedure is extremely effective, has no significant side effects and can be removed entirely in many cases as the student’s behavior improves
- JRC’s positive behavioral program is so effective that the skin shock procedure is currently being used for only 43 percent of JRC’s school-age students
- JRC’s treatment enables its students to do the following: stop taking harmful psychotropic drugs; avoid restraint, seclusion, warehousing and takedowns; avoid having to be placed in psychiatric hospitals or arrested by police for aggression and other destructive behaviors; start learning in school for the first time in their lives; avoid death or self-maiming by receiving effective and rapid treatment of self-abusive behaviors; have hope and optimism for their future where previous there was none; and enjoy the company of their parents and family for the first time in years.
Additional Comments from Matthew Israel
- The title page sets the tone of the article by referring to JRC as a “School of Shock.” The overwhelming reliance at JRC is on positive rewards and educational programs and ninety nine percent or more of a student’s time is spent in educational and rewarding experiences. Less than half of the school-age students at JRC have parent- and court-approved supplementary skin shock as a possible treatment option in their treatment programs. Those that do receive an average of one harmless (no significant side effects) two-second application to the surface of the skin, usually of the arm or leg, per week. As time goes on, many are able to graduate completely from needing this therapy.
- The title page contains the phrase “Food Deprivation.” Food deprivation is never used as a punishment at JRC. In the case of a small number of students food is used, with full parental and court approval, in the form of “mini-meals” that are earned as rewards in the the training of new skills. When this is done, elaborate steps are taken to either provide make-up meals at the end of the day or to otherwise insure proper nutrition and avoid any weight loss.
- The title page contains the word “Isolation.” Isolation is never used as a punishment at JRC.
- The title page says “Treats American kids like enemy combatants.” This statement, like the cover material and drawing, reflects an attempt to sensationalize JRC’s treatment and evidences a refusal to recognize the use of supplementary aversives as a scientifically proven and accepted form of behavioral treatment.
- The cover page shows a child in an Abu Ghraib torture-type position on a box with wires leading from the hands. Skin-shock is never used at JRC in the manner depicted in that drawing and is never used for the purpose implied (torture). Skin-shock is used at JRC as one small part of a behavior modification treatment program, based overwhelmingly on positive rewards and educational procedures, to help save and extend lives, to take students off of psychotropic drugs, and to help youngsters turn their lives around. Students whose problematic behaviors were so great that they were expelled or refused admission to every other available school, and who were headed for a prematurely short or miserable life of drugs, restraint and warehousing in a psychiatric hospital, in an institution, in a jail or on the streets are, through effective education and treatment at JRC based on scientifically-validated behavior modification procedures, given hope and optimism for their future where previously they had none. To compare this with Abu Ghraib-type torture is like equating a surgeon’s use of a knife in life-saving surgery to a felon’s use of a knife in a murderous stabbing.
- JRC has a unique set of rewarding features that is found in no other program. These rewards start with beautifully decorated school buildings that make coming to school a visually interesting and rewarding experience (many of our students have refused to attend school in the past). It continues with: an arcade-type Rewards Lounge; a “retail store” where students can purchase attractive personal items with the money they earn each week by displaying appropriate behaviors and learning; a lounge/reward corner in many classrooms; a reward afternoon once per week; Reward Boxes in many classrooms that contain desired items that students can earn each day; a personal computer and self-instructional software for every student; frequent field trips used as rewards; healthy and nutritional foods and no junk foods and soda machines; health-club type exercise facilities; community residences with wide-screen televisions, stereos and electronic games; and an open visiting policy in which parents or visitors can visit at any time of the day or night. To imply that a program that does all this for its students and parents is similar to the Abu Ghraib prison, as the cover and text of this article does, is to perpetuate a journalistic fraud on the readers.
- The article devotes the initial two pages to two former students whose parents changed their minds and decided to remove their son from JRC. JRC parents are always free to change their minds and withdraw their consent to JRC to employ aversives with their child. In both of the cases Ms. Gonnerman describes, the students made major progress while they attended JRC (a fact not reported by Ms. Gonnerman), and were removed prematurely before their treatment had been completed. The overwhelming majority of JRC parents have been extremely positive about JRC and thankful for the changes they have seen in their children. The fact that the first two pages focus on two former parents or students who have no verifiable evidence that the JRC program caused them any harm is further evidence of the bias that pervades the article.
- “To change their behavior, he developed a large repertoire of punishments…” Here, as in the article as a whole, there is a failure to give adequate space to JRC’s innovative and wide-ranging use of rewards and educational procedures, which is the background against which aversives are introduced, if needed in some cases, as an occasional (once per week, on average) supplement in the programs of a minority of our school-age students. No mention is made of the fact that all of these aversive procedures were parent- and court-approved.
- Ms. Gonnerman discusses California student Danny Aswad’s death as though it had something to do with JRC or me. It did not. JRC had ceased its operations in California a year or two prior to this student’s death which was from natural causes.
- “Three quarters of the articles were published more than 20 years ago…” Ms. Gonnerman fails to explain that the reason for the decrease in the number of recent professional articles dealing with skin-shock is that the procedure has become increasingly controversial during the last few decades. During the past 10 years, however, five papers involving the clinical use of skin shock, or reviewing research in which skin shock has been used, have appeared in the professional literature
- Ms. Gonnerman presents negative comments about JRC or me from three psychologists, Drs. Axelrod, Iwata and Touchette. One of these (Dr. Touchette) has never visited JRC and the others (Drs. Iwata and Axelrod) have not visited JRC during the last 12 and 18 years respectively. Ms. Gonnerman never asked me to provide her with the names of psychologists who support the use of aversives and who have taken the time to visit the current JRC program and observe our current treatment at first-hand.
- In a sidebar that appears on the Mother Jones web site, but not in the printed article, Dr. Iwata criticizes us for not using his approach to functional analysis/assessment. We are aware of Dr. Iwata’s approach and have tried it at JRC. The main problem is that the students who come to JRC have, by and large, already had the benefit of extensive functional analysis/assessment and despite this still have major behavior problems that were not solved with this approach alone. In that respect the situation is similar to the use of psychotropic drugs—the students who come to JRC have already been treated with psychotropic drugs and the drugs have been found insufficient. Despite this, JRC does do a comprehensive functional assessment of each student and takes the results into account in designing a program for the student and in designing the general treatment procedures employed in JRC’s program. In a comprehensive review of the literature on Positive Behavior Support, an approach that is opposed to the use of aversives, Carr et al found that the studies that use positive-only treatment procedures, even when functional analysis is included, were effective in only 60 percent of the cases. JRC’s population is largely taken from the remaining 40 percent.
- Ms. Gonnerman incorrectly states that the only time that JRC students can socialize freely is in the Big Reward Store. This is not true. There are many other places where students can socialize with each other such as on the playground, on field trips, at their residences, etc. They are not allowed to socialize with each other in the classroom, however, which is the rule in most schools.
- A former teacher, Jessica Croteau, complains of the fact that a lot of the education at JRC takes place through self-instructional software and personal computers. This is a very valuable application of behavioral psychology to education and is probably unique to JRC, where each student is given his/her own computer. Most of our teachers, parents and students value this self-instructional aspect of the program very much, which is provided in addition to classroom discussion. Their point of view was not presented. Why did Ms. Gonnerman not interview some former teachers who are positive about our program?
- Former student Rob Santana made great progress while at JRC which was a huge improvement when compared to his plight prior to his admission to JRC. It is unfortunate that Rob’s parent chose to remove him from JRC prematurely and it is unfortunate that he has been arrested and jailed since his discharge from JRC.
- Ms. Gonnerman complains that she did not have the opportunity to speak privately with JRC’s students. She never asked for such opportunities.
- Ms. Gonnerman objects to the fact that direct care staff members are not given the authority and flexibility to decide when to apply skin shocks and when not to. But to allow that to happen would mean that the treatment would not be applied consistently as it must be in order to be effective. More importantly, to allow that would be similar to allowing nurses in a hospital to decide whether and how much medication should be administered, instead of keeping such decisions under the control of the supervising physician. Direct care staff at JRC are encouraged and required to convey suggestions and concerns about treatment to the student’s treatment team at JRC, but the final decision as to what behaviors need to be treated with an aversive, and when this treatment should be administered, is properly placed under the control of the supervising clinician.
- Ms. Gonnerman objects to the fact that JRC discourages staff members from socializing with each other while on duty. It is vital, however, that the staff members give their undivided attention to the students. If a staff member socializes with other staff members when he or she should be attending to the students, this can create an unsafe situation.
- Ms. Gonnerman interviewed eight former staff members who were critical of how the GED was used. These alleged witnesses have no credibility because they refused to be identified. Furthermore, how did she happen to choose these former staff members and why did she not interview some of the many former staff members who are not critical? She did not ask JRC to recommend any former or current employees for possible interviews.
- Ms. Gonnerman makes much of the June 2006 New York State Department of Education Report that contained numerous criticisms of JRC. She fails to mention the fact that subsequent to that report three Massachusetts agencies have investigated JRC and found no support for the major findings of that report.
- The squib about Ms. Gonnerman characterized her article as resulting from a “yearlong investigation.” In fact her “investigation” was both brief and one-sided. She spent only two days visiting JRC in September of 2006 and did not witness even a single application of skin-shock to a student (despite giving the incorrect impression in her article that such applications are frequent occurrences). She went to great lengths to interview hostile former parents, teachers and staff (eight disgruntled former staff members—one for eight hours—out of thousands of possible former JRC staff members). She failed to interview any former parents, teachers and staff members with favorable opinions about JRC. Ms. Gonnerman devoted 10 column inches to describing students who died from natural causes entirely unrelated to their treatment (one 26 years ago and not even a JRC student, one 22 years ago, and one 17 years ago), but no column inches at all to students whose lives have been saved by JRC’s treatment procedures and no column inches to the case of a former JRC student (a case that I brought to her attention) who died from inadequately treated self-abuse when he was abruptly transferred from JRC to a program that used positive-only procedures.
She failed to inform the reader that all large treatment facilities for the severely disabled experience deaths, especially facilities like JRC that have been in operation for over 35 years and that treat the most fragile and dangerous population. JRC actually has experienced very few deaths, all of which were investigated by the proper state authorities, and none of which were found to be caused by JRC’s treatment program. She devoted 36 column inches to three disgruntled former parents and only 4 inches to parents who are among the hundreds who are extremely favorable to JRC. We heard no reports of her speaking to any supportive JRC parents other than the few that she interviewed for an hour or two during her visit to JRC.
Ms. Gonnerman’s article was originally written for the New York Times Sunday Magazine. The Times rejected it, a fact that she learned in early April of this year. She then apparently tried to find some other magazine which would buy the article. Consequently, much of the so-called “year-long investigation” was probably spent in trying to find a magazine willing to publish such a biased story.
- Ms. Gonnerman’s objective (which the Mother Jones editors joined in on) was apparently to incite opposition to JRC and agitate for laws to prohibit aversives. At least one mother was not persuaded as evidenced from this email that was sent to the JRC website recently.
EDITORS’ RESPONSE TO MATTHEW ISRAEL REGARDING “SCHOOL OF SHOCK”
THE USE OF SKIN SHOCK
In support of JRC’s use of skin shock, Israel and his defenders stress the violent and self-abusive behavior of some students, and argue that those students have not benefited from other forms of treatment. Israel writes: “It is well documented in scientific articles and in court findings that some special needs children and adolescents have behaviors that are so self-abusive, aggressive or destructive as to be life-threatening and self-maiming.”
The facts:
The use of skin shock is not restricted to such “low functioning” students. A report of an investigation by the New York State Education Department states, “JRC employs a general use of Level III aversive behavioral interventions [which include skin shock] to students with a broad range of disabilities, many without a clear history of self-injurious behaviors. JRC employs a general use of Level III aversive behavioral interventions to students for behaviors that are not aggressive, health dangerous or destructive.”
THE DEATH OF A STUDENT
Israel writes:
“Ms. Gonnerman discusses California student Danny Aswad’s death as though it had something to do with JRC or me. It did not. JRC had ceased its operations in California a year or two prior to his death which was from natural causes.”
The facts:
According to the 1982 complaint filed by the State of California, this student was in the care of the Behavior Research Institute at the time of his death. The complaint states that the student died while in restraints that kept him flat on his stomach in bed, and had been restrained on numerous occasions over the preceding seven months, despite the fact that such restraint was “contraindicated” because he suffered from a circulatory disorder. Dr. Israel helped found the Behavior Research Institute in California, which was a branch of the entity by the same name that he founded in Rhode Island (later renamed as JRC). Dr. Israel was a consultant to the Behavior Research Institute at or at least shortly before the time the student died. Dr. Israel has previously defended the Behavior Research Institute, saying that the death was not the result of treatment.
DR. IWATA’S VISIT
Israel writes:
“Her statement that Dr. Iwata has visited the Rotenberg Center is false.”
The facts:
Dr. Iwata visited the Rotenberg Center to review its practices at the request of Massachusetts officials. A copy of the report he wrote in 1995 was obtained by Mother Jones. At the time, the Rotenberg Center was still located in Rhode Island, but it already employed the skin shock aversive treatment that it still uses today.
SOCIALIZING AND ISOLATION
Israel writes:
“Ms. Gonnerman incorrectly states that the only time that JRC students can socialize freely is in the Big Reward Store. This is not true. There are many other places where students can socialize with each other such as on the playground, on field trips, at their residences, etc.”
The facts:
In an interview with Jennifer Gonnerman, Dr. Israel stated, “We need to marshal every possible reward you can find to reward desired behavior. So even opportunities for some of the high functioning students to socialize with other students or staff, instead of those being routinely provided, those actually have to be earned. Everything you want has to be earned.” The report by the New York State Education Department states, “During five observations involving a total of 59 students, there were no instances of students socializing with other students and only five instances observed of students socializing with staff. Social interactions between students reportedly occur in the Big Reward Store where students go to select a reward for keeping contracts. When questioned about friendships and social interactions among students, the students interviewed stated that they were unable to socialize in a natural way.”
Israel writes:
“The title page contains the word ‘Isolation.’ Isolation is never used as a punishment at JRC.”
The facts:
Again, Dr. Israel himself has confirmed that some students must earn the opportunity to socialize with other students or staff. A report of an investigation by the New York State Education Department says that students may be restrained on four-point restraint boards or in chairs “for extensive periods of time (e.g. hours or intermittently for days).” Students are sometimes confined to “conference rooms,” which in some cases isolate them from everyone except a single staff member.
FOOD DEPRIVATION
Israel writes:
“The title page contains the phrase ‘Food Deprivation.’ Food deprivation is never used as a punishment at JRC.”
The facts:
According to JRC, about 10 percent of the students are in a “Contingent Food Program” or a “Specialized Food Program.” These programs require students to meet behavioral requirements in order to earn food. The New York State Education Department report says that students must “earn” meals by not displaying certain behaviors, and that if they do not they are “made to throw a predetermined caloric portion of their food into the garbage.”
Students in the Contingent Food Program are given “make-up meals” at the end of each day, but according to JRC “make-up food is deliberately intended to be an unattractive option.” Students in the Specialized Food Program do not receive “make-up food” unless they have eaten less than 26 percent of their normal daily caloric target. These programs are part of the court-approved treatment plans for the students, and students’ weight is monitored. The program is altered or suspended if the student drops below a certain weight.
According to the New York State Education Department report, “The Contingent Food Program and Specialized Food Program may impose unnecessary risks affecting the normal growth and development and overall nutritional/health status of students subjected to this aversive behavior intervention.”
USE OF OTHER THERAPIES BEFORE SHOCK TREATMENT
Israel writes:
“Before JRC uses aversives with any student, positive and educative procedures are tried for an average of 11 months to try to change serious problematic behaviors.”
The facts:
The article does not assert that other treatments are not tried before aversives are used. However, according to the New York State Education Department report, “JRC may decide prior to a student’s acceptance into the program that he/she requires aversive procedures based on historical and current behavioral information provided by parents, the CSE and other records/reports.” In addition, in some cases, “the use of aversive procedures may be a condition of the student’s acceptance and continued enrollment in the program.” Letters from parents of students at JRC appear to support these findings.
SAFEGUARDS
Israel writes:
“There are many safeguards at JRC to make sure that the skin-shock procedure is used carefully, professionally and properly. They include prior parental consent, prior individualized court authorization (the judge appoints an attorney to represent the child’s interests in this process), prior approval by a Human Rights Committee and a Peer Review Committee, clearance from a physician and a psychiatrist to insure that there are no medical contraindications, etc.”
The facts:
The article discusses parental and court consent, and expressly reports that court approval is required in all cases. (Attorneys who have represented students in approval proceedings have told Mother Jones that court approval is routinely granted, sometimes over their objections.) The article doesn’t suggest that other safeguards are not also employed in deciding to use or in monitoring the use of skin shock treatment. However, some of the procedures are apparently required as the result of JRC’s settlement with the State of Massachusetts, and according to the New York State Education Department report, “the integrity of the behavioral programming at JRC is not sufficiently monitored by appropriate professionals at the school and in many cases the background and preparation of staff is not sufficient to oversee the intensive treatment of children with challenging emotional and behavioral problems.”
FADING OUT SKIN SHOCK TREATMENT
Israel writes:
“As time goes on, many [students] are able to graduate completely from needing this [skin shock] therapy.”
The facts:
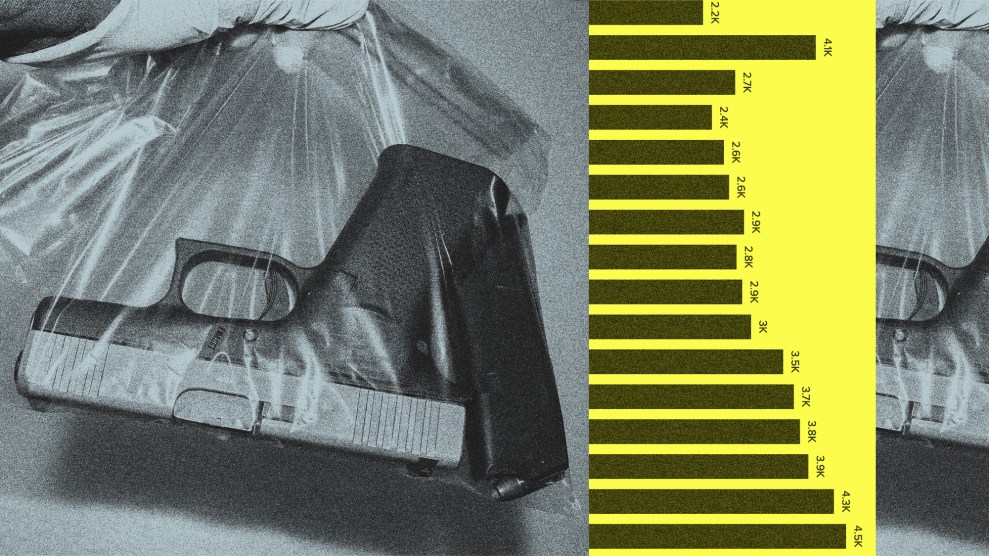
Data provided by Israel indicates that 43% of school-age students are receiving skin shocks, while only 3% percent have “graduated” or been “faded off” the shock devices. Among adult residents, 85% are attached to the shock device, while only 6% have been “faded off.” According to the New York State Education Department report, “JRC’s policy states, ‘GED fading will not occur until the student has gone a minimum of one year with no major behaviors.’…The criterion of one year without a ‘major disruptive behavior’ is extremely long and is not determined based on the circumstances for each individual student…Many NYS students remain on the GED for the entire time they attend the center.”
—Monika Bauerlein and Clara Jeffery